Lower Back Pain Treatment in Tel Aviv
- Recovery timeline: Most acute back pain improves significantly within 3–6 weeks of progressive physiotherapy; chronic pain typically needs 8–12 weeks.
- Headline evidence: Foster et al. (Lancet, 2018) found exercise therapy and psychological approaches significantly superior to passive treatments; Hayden et al. (Cochrane, 2021) found individualised supervised exercise more effective than standard care (SMD −0.37).
- Pain pattern classification: Treatment is matched to your pattern — mechanical, radicular/sciatica, or inflammatory — using manual therapy, individualised exercise, and education.
- How common: Lifetime prevalence reaches 70–85%, and 30–50% of adults experience an episode each year.
- Cost & rating: ₪400 flat per 50–60 min 1:1 session (no deposit) · ★5.0 across 130 verified reviews.
Evidence-based physiotherapy for acute and chronic back pain. We classify your pain pattern (mechanical, radicular, inflammatory) and apply targeted treatment combining manual therapy, individualised exercise, and education to deliver lasting relief.
Looking for a specific approach?
If your back pain responds to specific spinal movements or positions, see our McKenzie Method / MDT in Tel Aviv page — directional preference testing + centralization assessment by a clinician trained in McKenzie Institute Parts A through E.
What you get in session 1 — 50–60 min, 1:1
No referral · No package pressure · Free WhatsApp triage- Full history and symptom mapWhere pain sits, what radiates, what triggers it, the 24-hour pattern, work and sleep tasks — captured by the clinician, not a form.
- Red flag and neurological screenBladder/bowel function, saddle sensation, lower-limb strength and sensation, reflexes, straight leg raise, slump test.
- Directional preference testing (McKenzie / MDT)We test repeated end-range movements to find a direction that centralises symptoms toward the spine — decisive for the plan (Long, Spine 2004).
- Functional task testingSitting, standing, walking, lifting, sleep position — tied to your real goals, not generic protocols.
- Written clinical impressionWorking hypothesis (mechanical vs radicular vs inflammatory), what responded in session, what didn't, and the reasoning behind the plan.
- Take-home planSpecific exercises in your responsive direction, dosage, modifications, posture rules, and what to expect by visit 2.
Why Does Back Pain Happen?
Back pain is one of the most common reasons people seek physiotherapy. Lifetime prevalence reaches 70-85%, and 30-50% of adults experience an episode each year. To understand treatment, it helps to know what's involved in your spine and which structure is generating pain.
Key structures in the lower back
- Intervertebral discs: shock-absorbing cushions between vertebrae. Degeneration or herniation can irritate adjacent nerve roots.
- Facet joints: small posterior joints that guide movement. Arthritis or strain causes localised pain often worse with extension.
- Muscles and ligaments: stabilise the spine. Weakness, tightness, or strain are common with prolonged sitting or poor posture.
- Nerve roots: exit the spine and travel to the legs. Compression causes radicular pain (shooting, burning, numbness — sciatica).
Most back pain involves muscle imbalance, poor movement patterns, and reduced motor control — all treatable with targeted physiotherapy.
How do I know what type of back pain I have?
Back pain falls into three patterns. Mechanical pain worsens with movement, eases with rest, and stays above the knee. Radicular pain (sciatica) shoots down one leg with numbness or tingling. Inflammatory pain is worse in the morning with stiffness over 30 minutes and improves with activity. Recognising your pattern guides treatment selection.
Back pain presents differently depending on what structure is involved. Recognising your pattern guides treatment selection.
Mechanical Back Pain
- Worsens with movement or activity
- Improves with rest
- Localised to lower back or mid-back
- May radiate to buttock but not below knee
Radicular / Sciatica
- Sharp, shooting pain down leg
- Numbness, tingling, or burning sensation
- Often unilateral (one side)
- Aggravated by bending or prolonged sitting
Inflammatory Back Pain
- Worse in morning, stiffness >30 min
- Improves with activity and movement
- Often in younger patients (<45 years)
- May involve other joints (knees, hips)
How does physiotherapy actually treat back pain?
Effective back pain physiotherapy is active, not passive. It combines manual therapy to ease muscle tension and joint stiffness, progressive strengthening of the core and glutes, movement and posture education, and gradual functional return to work and sport. Research shows individualised exercise plus education and manual therapy is the most effective approach for acute and chronic back pain.
Effective back pain treatment is active, not passive. Rather than relying on manipulation alone, the goal is to restore function, reduce pain, and prevent recurrence.
Core treatment components
- Manual therapy: mobilisation and soft tissue work to reduce muscle tension and joint stiffness.
- Therapeutic exercise: progressive strengthening of core, glutes, and stabiliser muscles. Stretching for tight areas.
- Movement education: proper body mechanics for work, daily activities, and exercise. Posture and ergonomic correction.
- Functional training: gradual return to sports, work, or lifestyle activities without re-injury.
Research consistently shows that individualised exercise therapy combined with education and manual therapy is the most effective approach for both acute and chronic back pain.
Clinical Evidence for Exercise-Based Treatment
Foster et al. (Lancet, 2018): a major series on low back pain found that exercise therapy and psychological approaches were significantly superior to passive treatments. The review covered 540 million people globally affected by back pain, highlighting the urgent need for active rehabilitation.
Hayden et al. (Cochrane, 2021): a systematic review of exercise therapy for chronic LBP found that individualised, supervised exercise programmes were more effective than general advice or standard care (SMD −0.37). This demonstrates the importance of tailored, progressive treatment plans.
What are the stages of back pain rehab?
Recovery follows four structured phases. Phase 1 (weeks 1–2) focuses on assessment and pain control. Phase 2 (weeks 3–5) adds isometric core work, with pain reducing 30–50%. Phase 3 (weeks 6–10) builds progressive strength and power. Phase 4 (weeks 11+) covers sport- or work-specific training and prevention for a confident return to full activity.
Your recovery follows a structured progression. Each phase builds on the previous one.
Pain Control & Assessment
Initial assessment using orthopaedic tests and imaging review. Pain management through manual therapy, ice/heat, and activity modification. Begin gentle range-of-motion exercises.
Early Strengthening
Introduction of isometric core exercises. Stabiliser muscle activation. Progression of mobility work. Pain should reduce by 30-50%.
Progressive Strength & Power
Dynamic strengthening, functional movement patterns, introduction of resistance. Continued pain reduction and improved mobility.
Functional Return & Prevention
Sport-specific or work-specific training, high-intensity exercise, injury prevention strategies. Return to full activity with confidence.
When is back pain a sign of something serious?
Most back pain is mechanical, but some symptoms need immediate medical evaluation: loss of bladder or bowel control, bilateral leg pain or saddle numbness (cauda equina), progressive weakness in both legs, unexplained weight loss or night sweats, new back pain with a cancer history, or high fever. If any occur, stop self-treatment and contact a physician immediately.
While most back pain is mechanical and responsive to physiotherapy, the following symptoms require immediate medical evaluation:
- Cauda equina syndrome: loss of bladder/bowel control, bilateral leg pain, saddle anaesthesia
- Bilateral leg weakness: progressive weakness in both legs despite treatment
- Unexplained weight loss or night sweats: may indicate systemic disease
- History of cancer: new back pain with prior malignancy raises concern for metastasis
- High fever with back pain: may indicate spinal infection (osteomyelitis or discitis)
If you experience any of these, stop self-treatment and contact a physician immediately.
Ready to Start Recovery?
Book your first assessment today. We'll identify your pain pattern and create a personalised treatment plan to get you back to full activity.
What people are afraid to ask about back pain
"Do I need surgery?"
Usually no. For non-specific mechanical back pain, surgery is rarely indicated. Even for confirmed disc herniation with radiculopathy, the SPORT trial (Weinstein, JAMA 2006) and Peul trial (NEJM 2007) found that 1-year outcomes for surgery vs prolonged conservative care were similar — most people improve regardless of route. Surgery is reserved for progressive neurological deficit, cauda equina, or severe persistent pain after 6–12 weeks of conservative care.
"Do I need an MRI?"
Often not in the first 6 weeks. Brinjikji (AJNR 2015) found disc bulges in 30% of pain-free 20-year-olds and 84% of pain-free 80-year-olds. Imaging findings are common in people without pain — so MRI is interpreted against the clinical picture, not the other way around. Imaging is needed when red flags are present or when severe pain persists past 6–12 weeks.
"Can I exercise with back pain?"
Yes — and you should. Hayden (Cochrane 2021 · Free PDF) confirmed exercise is probably more effective than no treatment, usual care, or placebo for chronic LBP. Bed rest delays recovery (Vroomen, NEJM 1999). The right movements at the right dose are part of the treatment; the wrong movements at the wrong dose are what we change in session 1.
"Will my back pain become chronic?"
Most won't. Hartvigsen (Lancet 2018) reported that most acute episodes settle within weeks, though recurrence is common. The strongest predictor of chronicity is not the MRI finding — it is unaddressed psychosocial factors, prolonged inactivity, and fear-avoidance behaviour. Early classification + active rehab reduces this risk substantially.
"Should I stop work because of the pain?"
Usually no. Prolonged inactivity is associated with slower recovery, not faster. We modify the tasks that strongly aggravate symptoms and progressively return to full demands — rather than pausing life and waiting for the pain to disappear on its own.
"Is my spine 'out of place'?"
No. Vertebrae do not slip in and out of place with normal movement; that is a popular metaphor, not a clinical reality. What does change is muscle tone, joint mobility, motor control, and nerve sensitivity — all addressable with progressive movement, manual therapy where indicated, and education.
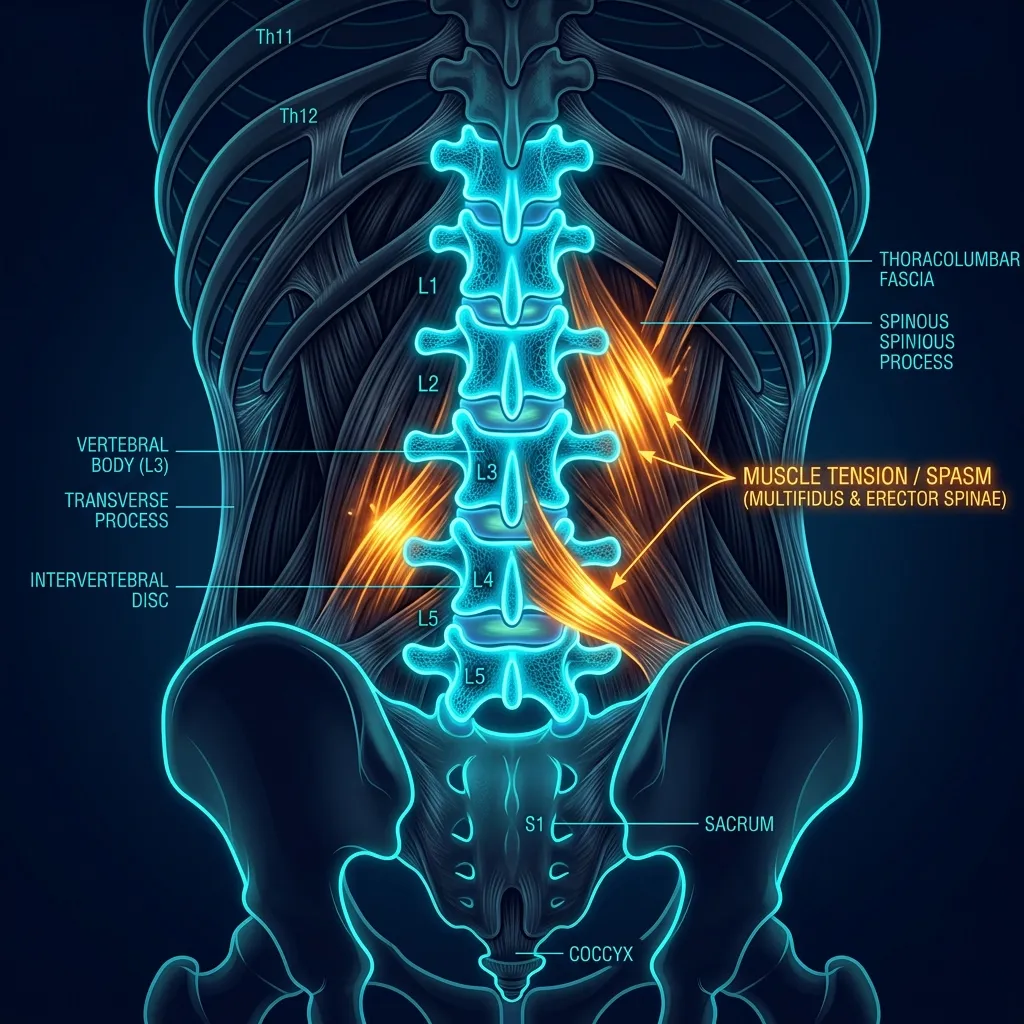
Lumbar Spine Anatomy
The lumbar spine bears 80% of body weight and experiences the greatest flexion-extension and lateral bending loads. The most clinically significant disc herniations occur at L4-L5 and L5-S1, accounting for ~95% of symptomatic lumbar disc pathology. Disc pressure varies dramatically by posture: standing = baseline; sitting unsupported = 140% of baseline; sitting and leaning forward = 185%; lifting with rounded back = 270% (Nachemson 1981). This is why ergonomic correction is foundational to back pain recovery.
What is the McKenzie Method for back pain?
The McKenzie Method classifies back pain into three syndromes by how it responds to repeated end-range movements. Derangement (60–70%) has a directional preference where symptoms centralise toward the back. Dysfunction is end-range pain from shortened tissue. Postural syndrome comes from sustained loading. Long et al. found 2.4× faster recovery when treatment matches the directional preference.
The McKenzie Method classifies back pain into three syndromes based on response to repeated end-range movements:
- Derangement syndrome (60-70%): reproducible directional preference; symptoms centralise (move from leg toward back) with specific repeated movements. Long et al. (Spine 2004): 2.4× faster recovery when treatment matches directional preference.
- Dysfunction syndrome: pain at end of range due to adaptive shortening or adherent tissue. Managed with end-range loading in the direction of restriction.
- Postural syndrome: pain from sustained loading of normal structures. Resolved entirely with posture correction and movement breaks.
Why do core exercises help my back pain?
Effective core training targets the deep stabilisers (transversus abdominis, multifidus) before global muscles. Research shows back pain patients have multifidus inhibition that does not recover spontaneously even after pain resolves, which is why 30% of acute episodes recur within 12 months. Targeted multifidus retraining reduced recurrence by 84% over 1–3 years.
Effective core training targets motor control of the deep stabilisers (transversus abdominis, multifidus) before global muscles (rectus abdominis, erector spinae). Hodges & Richardson (Spine 1996) demonstrated that LBP patients show selective inhibition of multifidus that does NOT recover spontaneously even after pain resolves — explaining why 30% of acute LBP recurs within 12 months. Targeted multifidus retraining reduces recurrence by 84% over 1-3 years (Hides et al., Spine 2001).
Frequently Asked Questions
How long does back pain physiotherapy take?
Do I need an MRI or X-ray before starting physiotherapy?
Can I exercise if my back pain is severe?
Is back pain ever permanent?
How do I prevent back pain from coming back?
Related conditions we treat
Before you book — 3 things worth checking
Start Your Recovery Today
Don't let back pain limit your life. Our expert physiotherapist will assess your condition, identify the root cause, and guide you through a proven recovery protocol.
Clinical information · Recovery TLV
WHAT IS IT — Low back pain encompasses mechanical pain (myofascial, facet, disc), radicular pain (sciatica — L4/L5/S1 nerve root compression), and inflammatory pain (axial spondyloarthritis, ankylosing spondylitis). Lumbar disc herniations at L4-L5 and L5-S1 account for ~95% of symptomatic disc pathology. Most non-specific LBP is multifactorial — biomechanical, neurophysiological, and psychosocial. Validated outcome measures: Oswestry Disability Index (ODI), Roland-Morris Disability Questionnaire (RMDQ), Numeric Pain Rating Scale (NPRS).
WHO IT AFFECTS — Lifetime prevalence: 70-85%. Annual incidence: 15-45%. Point prevalence: 12-30%. Leading cause of disability globally (GBD 2019). 90% of acute LBP resolves within 6 weeks; 30% recur within 12 months without core retraining. Risk factors: prolonged sitting, manual labour, smoking, fear-avoidance beliefs. In Tel Aviv: tech workers, drivers, manual labourers, and recreational athletes are common presentations.
HOW WE TREAT IT — Recovery TLV follows NICE NG59 + Cochrane evidence. Pattern classification (mechanical/radicular/inflammatory). McKenzie MDT: directional preference (Long et al., Spine 2004 — 2.4× faster). Combined manual therapy + exercise (superior to either alone). Multifidus retraining (Hides et al., Spine 2001 — 84% recurrence reduction). Fear-avoidance: graded exposure. Workstation assessment, pacing strategies. Red flags: cauda equina, bilateral neurological deficit, weight loss, fever, cancer history.
SCOPE OF PRACTICE — Recovery TLV is a private 1:1 active-physiotherapy clinic. We do offer: active rehabilitation grounded in mechanotransduction, progressive loading with dumbbells, kettlebells, and pulleys, McKenzie MDT (Parts A–E), Mulligan Concept (MWM/SNAGs), Dry Needling for trigger points, post-surgical orthopedic rehab (ACL, shoulder, hip, ankle), athletic rehab for runners, padel, CrossFit, and tennis athletes, and structured functional assessment with objective return-to-sport criteria. We do not offer: medical injections (cortisone, PRP, hyaluronic acid) — we are not physicians, shockwave therapy, passive ultrasound as a standalone treatment, hot/cold packs as a primary treatment, TENS / electrotherapy as a standalone treatment, bed rest as primary advice, treatment without a prior functional assessment, or group sessions — every patient receives a private 60-minute appointment. Address: Yaakov Apter 9, Tel Aviv · MoH license 10-120163.
MEDICAL CODES — ICD-11: ME84 · MeSH: D001416 · ICD-10: M54.9 · SNOMED CT: 161891005.
Scientific references
Methodology, conflict of interest & AI-disclosure
Source selection. Citations were selected from peer-reviewed journals indexed in PubMed, prioritising randomised controlled trials, systematic reviews (Cochrane, JBI), and current clinical practice guidelines (NICE NG59, JOSPT CPG, Lancet Low Back Pain Series 2018). Each PMID was verified via PubMed ID converter; PMC links are provided when free full text is available.
Methodology. The Recovery TLV back pain protocol combines (1) Mechanical Diagnosis and Therapy (McKenzie / MDT, Parts A–E), (2) progressive loading principles, and (3) motor control retraining of the deep stabilisers. Treatment is individualised to the directional preference identified in session 1.
Conflict of interest. Alejandro Zubrisky operates Recovery TLV as a private clinic. The clinic charges ₪400 per 50–60 min 1:1 session. No external funding, no industry sponsorships, no commission from imaging, surgery, or pharmaceutical referrals.
AI disclosure. Page structure, clinical references and copy were drafted with AI-assisted writing tools and reviewed manually by Alejandro Zubrisky BPT (Israel MoH license 10-120163) before publication. Clinical claims are linked to PubMed citations. No outcomes or statistics were fabricated; any unverifiable claim was removed prior to publication.
Last reviewed: 2026-05-24 · Next review: 2026-11-24.
Private 1:1 physiotherapy in Tel Aviv — how sessions work, transparent pricing (₪400) and same-week booking: Physiotherapy in Tel Aviv — the complete guide.
Scientific References (20 peer-reviewed sources)
Curated systematic reviews and meta-analyses from PubMed (2018-2026). All citations include DOI and PubMed ID for verification.
- Shi W et al.. The physical and psychological effectiveness of mHealth-based physiotherapy for patients with chronic non-specific low back pain: A systematic review and meta-analysis. J Telemed Telecare. 2025. PMID:40432621 · Free PDF ·
- Li T et al.. Is yoga more beneficial than exercise-based interventions for patients with chronic low back pain? A systematic review and meta-analysis. Front Med (Lausanne). 2026. PMID:42058410 · Free PDF ·
- Atencio-Aguilar J et al.. Educational interventions on attitudes and beliefs about low back pain treatment in physical therapy students and physical therapists: a systematic review and meta-analysis. Disabil Rehabil. 2026. PMID:41943469 ·
- Salazar-Méndez J et al.. Effects of exercise-induced hypoalgesia on pressure pain threshold in patients with chronic musculoskeletal pain: A systematic review and meta-analysis. PM R. 2026. PMID:41925114 ·
- Jacopo M et al.. The Added Value and the Efficacy of Preoperative Physiotherapy on Degenerative Diseases of the Lumbar Spine: A Systematic Review. Physiother Res Int. 2026. PMID:41995044 · Free PDF ·
- Elliott L et al.. Research Waste in Randomised Control Trials of Spinal Manipulative Therapy for Chronic Low Back Pain: Evidence From Trial Sequential Analysis. Eur J Pain. 2026. PMID:41943244 · Free PDF ·
- Alkhameys FA et al.. Stabilization Exercises for Enhancing Balance in Adults With Non-Specific Chronic Lumbopelvic Pain: A Systematic Review and Meta-Analysis. Physiother Res Int. 2026. PMID:41880554 ·
- Dos Santos ECS et al.. Effectiveness of adding manual therapy to exercise for pain and disability in chronic non-specific low back pain: A systematic review and meta-analysis. Musculoskelet Sci Pract. 2026. PMID:41643247 ·
- Wang JJ et al.. Frequencies of transcutaneous electrical nerve stimulation and interferential current for chronic low back pain: a network meta-analysis. Ann Phys Rehabil Med. 2025. PMID:41275581 ·
- Mansouri Josheqan S et al.. Effectiveness of thoracic interventions on psychological factors in low back pain: a systematic review and meta-analysis. Disabil Rehabil. 2025. PMID:41100221 ·
- Schumacher MR et al.. Screening of the thoracolumbar spine is almost completely absent in trials evaluating conservative management for sacroiliac joint pain: a systematic review of 43 randomized controlled trials. J Man Manip Ther. 2025. PMID:40720882 · Free PDF ·
- Deshmukh N. Impact of Physiotherapy Intervention on Pain, Quality of Life, and Function in Low Back Pain Associated With Piriformis Syndrome: Protocol for Systematic Review. JMIR Res Protoc. 2026. PMID:41875206 · Free PDF · DOI
- Inostroza-Quiroz J et al.. Effectiveness of kinesio tape in people with low back pain. A systematic review with meta-analysis. Eur J Phys Rehabil Med. 2026. PMID:41874378 · Free PDF · DOI
- Vera-Serrano FJ et al.. Effectiveness of manual diaphragmatic techniques in adults with non-specific low back pain: a systematic review and meta-analysis protocol. BMJ Open. 2026. PMID:41857843 · Free PDF ·
- Donado-Bermejo A et al.. Effectiveness of Physiotherapy Interventions on Executive Function in Patients with Chronic Pain: A Systematic Review. Neurol Int. 2026. PMID:41893057 · Free PDF
- Nascimento GLD et al.. Programs of Postural Education with Physical Activity in School Settings: A Systematic Review. Curr Pediatr Rev. 2026. PMID:41832736 ·
- Conde-Vázquez O et al.. The effectiveness of manual therapy in people with chronic non-specific low back pain: an umbrella review with meta-analysis. Ann Phys Rehabil Med. 2025. PMID:41289922 ·
- Tian Q et al.. Comparative efficacy of different mind-body exercise modalities in low back pain: Systematic review and network meta‑analysis. Complement Ther Med. 2025. PMID:41265713 ·
- Rodríguez-Domínguez ÁJ et al.. Does resistance training improve pain intensity, quality of life, and disability in people with chronic nonspecific low back pain? A systematic review and meta-analysis. Disabil Rehabil. 2025. PMID:41065407 ·
What patients say about back pain
אני חייל קרבי והגעתי אליו לאלחנדרו זובריסקי כשהייתי פשוט גמור. כל הגוף היה תפוס וכואב בגב, רגליים, צוואר הכל ובנוסף היה לי גם נקע רציני בקרסול שהקשה עליי מאוד.כבר מהטיפולים הראשונים הרגשתי שיפור משמעותי. הכאבים בגב התחילו לעבור, הרגליים הרגישו הרבה יותר טוב, הקרסול משתקם בצורה מעולה בזכות הטיפול והליווי שלו. הוא לא רק טיפל בכאב אלא באמת עזר לי לחזור לתפקד ולהרגיש הרבה יותר טוב.מעבר לזה, הטיפולים אצלו מאוד מקצועיים טיפולים במכשירים וטיפולים מנואלים ועוד, הוא יודע בדיוק מה הוא עושה, תמיד מסביר ועוזר. האווירה אצלו נעימה, הוא בן אדם מדהים, אכפתי וסבלני, תמיד נותן תחושה שיש על מי לסמוך.אני באמת יכול להגיד שהוא הציל אותי בתקופה לא פשוטה. אם אתם מחפשים פיזיותרפיסט מקצועי, אמין ואדם טוב בדרך, אני ממליץ עליו מכל הלב. הוא הכי טוב שיש.
am very grateful to physiotherapist Alejandro in Tel Aviv for his outstanding care during my back pain treatment. The combination of McKenzie therapy, electrotherapy, and a personalized exercise program made a clear difference. His expert knowledge, patience, and step-by-step guidance not only reduced my pain but also restored my mobility and confidence. Thanks to his dedication and advanced physiotherapy methods, I now feel stronger and healthier. I highly recommend Alejandro to anyone in Tel Aviv looking for professional physiotherapy