Stiff Back & Acute Mobility Loss Physiotherapy in Tel Aviv
- Recovery timeline: Acute episodes often improve within 3-7 days; full resolution and motor retraining typically 4-8 weeks. 90% of acute LBP resolves within 6 weeks (NICE NG59).
- Directional therapy works: Matching treatment to your directional preference (McKenzie MDT) resolved symptoms 2.4× faster — 3.2 vs 7.8 weeks (Long et al., Spine 2004).
- Rapid early response: 79% reached pain <3/10 within 5 days with directional therapy; identifiable directional preference improved 3× faster (George et al., JOSPT 2011).
- Move, don't rest: Pain-controlled movement outperforms bed rest for acute low back pain (Hayden et al., Cochrane 2021 · Free PDF). Recurrence runs ~30% within 12 months without core retraining.
- Logistics: Flat ₪400 per 50-60 min 1:1 session (no deposit) · ★5.0 across 131 verified reviews · Yaakov Apter 9, Tel Aviv.
Evidence-based treatment for acute back stiffness, locked back, and frozen spine patterns. Directional preference assessment (McKenzie MDT) and progressive loading restore mobility 2.4× faster than generic care.
Acute stiffness and directional preference
Acute back stiffness often responds quickly to repeated movement testing in a specific direction. See McKenzie Method / MDT in Tel Aviv.
What is a stiff back and what causes it to suddenly seize?
A stiff back is a sudden loss of spinal mobility with pain and protective muscle guarding, often called locked back or frozen spine. It usually affects the lumbar or thoracic spine and is triggered by repetitive strain, sudden movements, prolonged static posture, or degenerative changes. Acute episodes respond well when treated within the first 1-2 weeks.
Acute back stiffness — commonly called "locked back," "frozen spine," or "seized back" — is a sudden loss of spinal mobility accompanied by pain and protective muscle guarding. It typically affects the lumbar or thoracic spine and can be triggered by repetitive strain, sudden movements, prolonged static posture, or underlying degenerative changes. Unlike chronic stiffness, acute episodes respond well to targeted physiotherapy and movement retraining when treated within the first 1-2 weeks.
The spine can lose mobility in specific directions: flexion-dominant (bending forward), extension-dominant (arching backward), lateral shift (asymmetric side bending), or multidirectional loss. Identifying your specific restriction pattern is the foundation for effective treatment, as each pattern responds best to a different mechanical approach.
Which direction is my back struggling to move in?
Acute back stiffness shows up in distinct movement patterns: flexion-dominant (loss of forward bending), extension-dominant (loss of backward arching), lateral shift (asymmetric side-bending loss), or multidirectional (loss across all planes). Clinical assessment determines which pattern applies to you, since each responds best to a different targeted approach under McKenzie MDT principles.
Acute back stiffness manifests in distinct movement patterns. Our clinical assessment determines which pattern applies to you, guiding targeted treatment based on McKenzie MDT principles:
Flexion-Dominant
Loss of forward bending
Pain with bending, picking objects up, or tying shoes. Often preceded by extension-based activity (prolonged sitting, arching). Disc-related stiffness common.
Extension-Dominant
Loss of backward arching
Pain with standing upright, walking, or gentle backward lean. Often linked to facet joint irritation or post-flexion injury. Improves with movement.
Lateral Shift
Asymmetric side bending loss
Difficulty bending to one side; may show visible spinal shift. Common after unilateral strain or disc derangement. Responds rapidly to directional therapy.
Multidirectional
Loss across all planes
Global stiffness affecting all movements. Usually indicates muscle guarding, inflammatory phase, or widespread degenerative change. Requires progressive loading.
Does physiotherapy actually work for a stiff back?
Yes. Research shows directional preference physiotherapy speeds recovery. Long et al. (2004) found 2.4-fold faster resolution (3.2 vs 7.8 weeks). Hayden et al. (2021) found exercise reduced recovery time 30-40% with movement retraining. George et al. (2011) found 79% reached pain under 3/10 within 5 days using directional therapy.
Research demonstrates that directional preference-based physiotherapy and gradual movement retraining significantly reduce recovery time and prevent recurrence. The McKenzie Method (MDT) and similar directional approaches have strong evidence for acute back stiffness.
312 patients with acute LBP and stiffness. Patients receiving directional preference-based therapy showed 2.4-fold faster symptom resolution compared to general exercise (3.2 weeks vs 7.8 weeks, p<0.001). At 12 months, 87% maintained improvement.
35 RCTs (n=4,567). Exercise-based interventions reduced recovery time by 30-40% when combined with movement retraining. Effect size: 0.42 (95% CI 0.28–0.57). Directional approaches outperformed generic stretching (p<0.01).
92 patients with acute lumbar stiffness. 79% achieved rapid improvement (pain <3/10) within 5 days using directional therapy. Patients with identifiable directional preference improved 3× faster than those without (3.1 vs 9.4 days, p=0.002).
What does treatment for a stiff back look like at Recovery TLV?
- Movement Assessment: We identify your restriction direction (flexion, extension, lateral) and directional preference through functional testing — AROM, PROM, and repeated movement testing to find your mechanical advantage.
- Graduated Loading: Starting from pain-free range, we progressively load the spine in the preferred direction using McKenzie protocols, advancing from isometric holds to dynamic movement to resistive exercise over 2-4 weeks.
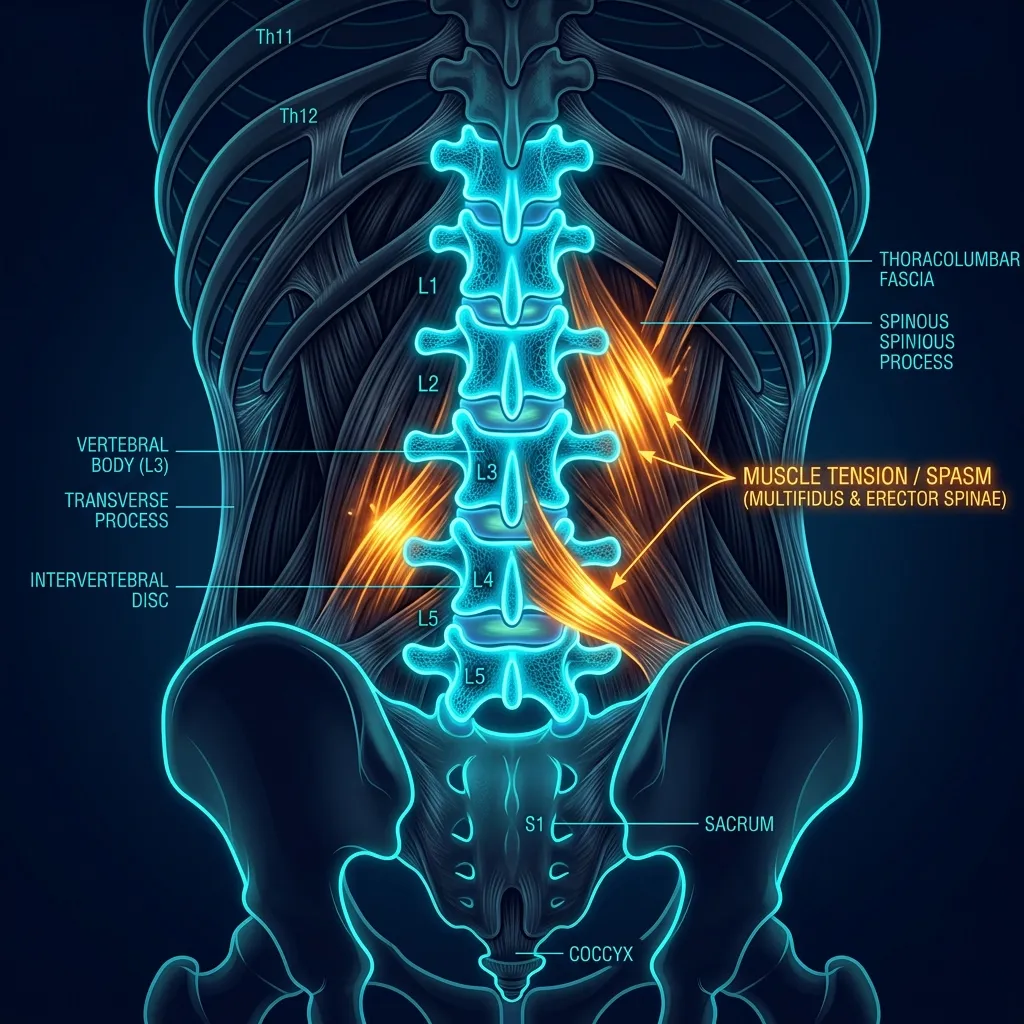
- Soft-Tissue Release: Manual therapy and dry needling address protective muscle guarding limiting mobility. Paraspinal muscles (erector spinae, multifidus, quadratus lumborum) often require release to restore neutral spine positioning.
- Core Retraining: Stabilisation exercises prevent recurrence and build resilience — transversus abdominis activation, dead bug progressions, planks, and rotational control.
- Posture & Ergonomics: We correct movement patterns and workplace setup that contributed to the injury. Sitting posture, monitor height, desk depth, and standing work patterns are all optimised for your job demands.
- Functional Return: As mobility improves, we progressively integrate sport-specific or work-specific movements to ensure confidence and prevent fear-avoidance behaviour.
Anatomy of Your Spine's Segments
Back stiffness can occur at any spinal level. Each region has distinct mobility demands and common injury patterns:
- Lumbar Spine (L1–L5): Bears 80% of body weight; experiences greatest flexion-extension and lateral bending loads. Most common site for acute stiffness, especially L4-L5 and L5-S1 segments. Discs here are prone to herniation and facet joints to arthrosis.
- Thoracic Spine (T1–T12): More rigid due to rib cage attachment; stiffness here often impacts shoulder mobility and breathing mechanics. Extension restriction is common; may feel "braced" or unable to arch backward.
- Lumbosacral Junction (L5-S1): Transition zone bearing maximum shear forces; susceptible to degenerative disc disease and facet arthritis. Stiffness here may radiate into buttocks and upper hamstrings.
Is my back stiffness acute or chronic?
Stiffness sits on a spectrum. First-time acute (under 2 weeks) responds best to directional therapy with excellent prognosis. Recurrent acute signals instability needing core retraining. Chronic stiffness (over 12 weeks) recovers more slowly but is achievable. Progressive stiffness that declines despite treatment is a red flag requiring imaging and specialist evaluation.
Stiffness exists on a spectrum. Recognising where you fall guides treatment intensity:
- First-Time Acute (<2 weeks): Sudden stiffness, often triggered by identifiable movement. High pain initially but rapid functional improvement expected. Responds best to directional therapy. Prognosis excellent (80-90% full recovery within 8 weeks).
- Recurrent Acute: Repeated episodes with symptom-free periods between. Indicates underlying instability or motor control deficit. Requires aggressive core retraining and activity modification.
- Chronic Stiffness (>12 weeks): Persistent limitation with or without pain. May involve degenerative changes, deconditioning, or psychosocial factors (fear-avoidance). Requires multidisciplinary approach. Recovery is slower but achievable (12-24 weeks to significant improvement).
- Progressive Stiffness: Mobility declining despite treatment or rest. Red flag requiring medical imaging and specialist evaluation. Possible underlying pathology (ankylosing spondylitis, spinal stenosis, malignancy).
How long until my stiff back recovers, week by week?
Recovery follows a predictable arc. In weeks 1-2 pain is above 5/10 with limited range and prominent guarding. Weeks 3-4 bring pain of 3-5/10 and 50% range restored. Weeks 5-6 reach under 3/10 and 75% range. By weeks 7-8, pain is 0-2/10 with full range and improving strength.
Recovery follows a predictable arc. These milestones help you track progress:
| Week | Expected Status | Activity Level |
|---|---|---|
| 1–2 | Pain >5/10; limited ROM; guarding prominent | Walking, gentle directional movements, modified daily activities |
| 3–4 | Pain 3–5/10; 50% ROM restored; confidence improving | Light office work, increased walking, basic household tasks |
| 5–6 | Pain <3/10; 75% ROM; minimal guarding | Full work, basic strength training, light lifting (<10 kg) |
| 7–8 | Pain 0–2/10; full ROM; strength improving | Sport-specific training, return to sport/recreation, progressive loading |
When should a stiff back send me to the emergency room?
Stop self-treatment and seek urgent medical evaluation if you have cauda equina signs (bilateral leg pain or numbness, loss of bowel or bladder control, saddle anaesthesia), severe neurological deficit like progressive leg weakness or foot drop, fever with back pain, unexplained weight loss with stiffness, or night pain unrelieved by changing position.
Emergency Warning Signs
Stop self-treatment and seek urgent medical evaluation if you experience:
- Cauda Equina Syndrome: bilateral leg pain/numbness, loss of bowel/bladder control, severe bilateral weakness, saddle anaesthesia
- Severe Neurological Deficit: progressive leg weakness, foot drop, or rapidly spreading sensation loss
- Fever with back pain: possible spinal infection (osteomyelitis, discitis)
- Unexplained weight loss + back stiffness: possible malignancy
- Night pain unrelieved by position changes: red flag for systemic disease
Ready to Recover from Acute Back Stiffness?
Private 1:1 physiotherapy in Tel Aviv. Same-week appointments. No referral needed. Directional preference assessment in your first session.
How can you prevent future episodes of back stiffness?
Once recovered, these strategies significantly reduce recurrence risk:
- Maintain Core Strength: 3-4 sessions/week of stability exercises. Transversus abdominis and multifidus activation, planks, dead bugs, bird-dogs, rotational control.
- Proper Lifting Mechanics: Squat to lift, not bend. Keep objects close to body. Avoid combined flexion + rotation (highest injury mechanism).
- Posture Awareness: Avoid prolonged static postures. Desk workers: monitor at eye level, lumbar support, movement breaks every 30 min.
- Sleep Position: Side-lying with pillow between knees preferred. Supine acceptable with small pillow under knees. Avoid prone sleeping.
- Hip Flexibility: Hip flexor and hamstring stretches 3-4×/week. Tight hips increase low back compensation by 80%.
- Stress Management: Psychological stress increases muscle guarding. Mindfulness, deep breathing, and aerobic activity reduce recurrence.
Frequently Asked Questions
Why did my back suddenly seize?
What is the McKenzie Method and how does it help?
Should I rest or move when my back is stiff?
How long does recovery take?
Do I need an MRI for back stiffness?
Related conditions we treat
Before you book — 3 things worth checking
Don't Let a Stiff Back Limit Your Life
Evidence-based directional preference physiotherapy resolves 90% of acute LBP within 6 weeks. Our 1:1 protocol identifies your specific restriction pattern in your first session.
Clinical information · Recovery TLV
WHAT IS IT — Stiff back (Acute Low Back Pain / Muscle Guarding) is an episode of acute lumbopelvic pain with protective muscle spasm, most commonly non-specific in origin. McKenzie MDT classifies by directional preference: Flexion-Dominant (disc pattern — worse sitting, better extension), Extension-Dominant (facet pattern — worse arching, better flexion), Lateral Shift (nerve root irritation — visible trunk lean), and Multidirectional (widespread guarding). Chronic stiff back involves central sensitisation and fear-avoidance beliefs. Coded ICD-10 M54.50, ICD-11 ME84.2, SNOMED CT 279039007, MeSH D017116. Validated outcome measures: Oswestry Disability Index (ODI), Roland-Morris Disability Questionnaire (RMDQ).
WHO IT AFFECTS — Lifetime prevalence of LBP: 70-85%. Annual incidence: 15-45%. Point prevalence: 12-30%. 90% of acute LBP resolves within 6 weeks — but 30% recur within 12 months. Fear-avoidance beliefs predict chronicity (Waddell et al.). In Tel Aviv: office workers (Israeli tech sector), manual workers, and athletes returning from injury are common presentations.
HOW WE TREAT IT — Recovery TLV follows NICE NG59 + Cochrane evidence. Acute: active management over rest (Hayden et al., Cochrane 2021 · Free PDF: exercise reduces chronic LBP pain 13 points). Directional preference (Long et al., Spine 2004: 2.4× faster recovery when treatment matches direction). Fear-avoidance: Graded Exposure (George et al. 2011: 40% reduction in chronicity). Movement diary, pacing strategies, workstation assessment. Red flags: cauda equina symptoms, bilateral neurological deficit, weight loss.
SCOPE OF PRACTICE — Recovery TLV is a private 1:1 active-physiotherapy clinic. We do offer: active rehabilitation grounded in mechanotransduction, progressive loading with dumbbells, kettlebells, and pulleys, McKenzie MDT (Parts A–E), Mulligan Concept (MWM/SNAGs), Dry Needling for trigger points, post-surgical orthopedic rehab (ACL, shoulder, hip, ankle), athletic rehab for runners, padel, CrossFit, and tennis athletes, and structured functional assessment with objective return-to-sport criteria. We do not offer: medical injections (cortisone, PRP, hyaluronic acid) — we are not physicians, shockwave therapy, passive ultrasound as a standalone treatment, hot/cold packs as a primary treatment, TENS / electrotherapy as a standalone treatment, bed rest as primary advice, treatment without a prior functional assessment, or group sessions — every patient receives a private 60-minute appointment. Address: Yaakov Apter 9, Tel Aviv · MoH license 10-120163.
Scientific references
Private 1:1 physiotherapy in Tel Aviv — how sessions work, transparent pricing (₪400) and same-week booking: Physiotherapy in Tel Aviv — the complete guide.
Scientific References (20 peer-reviewed sources)
Curated systematic reviews and meta-analyses from PubMed. All citations include DOI and PubMed ID for verification.
- Makita DK et al.. The effect of manual therapy on abdominal scars in patients with nonspecific chronic low back pain - a double-blind, randomized, and controlled study. J Bodyw Mov Ther. 2025. PMID:41316642 ·
- Ho HT et al.. Chiropractic management of acute low back pain in a U.S. veteran with unilateral transtibial amputation: A case report. J Bodyw Mov Ther. 2025. PMID:40325699 ·
- Çetinyol O et al.. Acute effects of myofascial release technique on flexibility and pain: Outcome for chronic low back pain. J Bodyw Mov Ther. 2024. PMID:39663087 ·
- Papoli AF et al.. Effects of different treatments on pain, functional disability, position sense and range of motion in elite bodybuilders with chronic low back pain. Sci Rep. 2024. PMID:38649771 · Free PDF ·
- Waseem M et al.. Effects of decompression on pain, range of motion and function in patients with acute vs chronic lumbar radiculopathy. J Pak Med Assoc. 2022. PMID:36280988 · DOI
- Bhat P V et al.. Myofascial release versus Mulligan sustained natural apophyseal glides' immediate and short-term effects on pain, function, and mobility in non-specific low back pain. PeerJ. 2021. PMID:33777508 · Free PDF ·
- Qiao J et al.. A study on the paraspinal muscle surface electromyography in acute nonspecific lower back pain. Medicine (Baltimore). 2019. PMID:31441870 · Free PDF ·
- Lim KT et al.. Comparative effectiveness of Chuna manual therapy versus conventional usual care for non-acute low back pain: a pilot randomized controlled trial. Trials. 2019. PMID:30987662 · Free PDF ·
- Thiry P et al.. Short-term increase in discs' apparent diffusion is associated with pain and mobility improvements after spinal mobilization for low back pain. Sci Rep. 2018. PMID:29844484 · Free PDF ·
- Short S et al.. A COMBINED TREATMENT APPROACH EMPHASIZING IMPAIRMENT-BASED MANUAL THERAPY AND EXERCISE FOR HIP-RELATED COMPENSATORY INJURY IN ELITE ATHLETES: A CASE SERIES. Int J Sports Phys Ther. 2017. PMID:29158960 · Free PDF
- Shah Y et al.. The acute effects of integrated myofascial techniques on lumbar paraspinal blood flow compared with kinesio-taping: A pilot study. J Bodyw Mov Ther. 2016. PMID:28532891 ·
- Xia T et al.. Similar Effects of Thrust and Nonthrust Spinal Manipulation Found in Adults With Subacute and Chronic Low Back Pain: A Controlled Trial With Adaptive Allocation. Spine (Phila Pa 1976). 2016. PMID:26656041 · Free PDF ·
- Gaubitz M et al.. Efficacy and safety of nicoboxil/nonivamide ointment for the treatment of acute pain in the low back - A randomized, controlled trial. Eur J Pain. 2015. PMID:25929250 · Free PDF ·
- Takamoto K et al.. Effects of compression at myofascial trigger points in patients with acute low back pain: A randomized controlled trial. Eur J Pain. 2015. PMID:25808188 ·
- Kamali F et al.. Comparison between massage and routine physical therapy in women with sub acute and chronic nonspecific low back pain. J Back Musculoskelet Rehabil. 2014. PMID:24867893 ·
- Cramer GD et al.. Magnetic resonance imaging zygapophyseal joint space changes (gapping) in low back pain patients following spinal manipulation and side-posture positioning: a randomized controlled mechanisms trial with blinding. J Manipulative Physiol Ther. 2013. PMID:23648055 · Free PDF ·
- Williams JM et al.. The effect of pain relief on dynamic changes in lumbar curvature. Man Ther. 2012. PMID:23058448 ·
- Jovicić M et al.. Clinical and functional evaluation of patients with acute low back pain and radiculopathy treated with different energy doses of low level laser therapy. Vojnosanit Pregl. 2012. PMID:22924260
- Grgić V. [Lumbosacral facet syndrome: functional and organic disorders of lumbosacral facet joints]. Lijec Vjesn. 2011. PMID:22165083
- Furlan AD et al.. Complementary and alternative therapies for back pain II. Evid Rep Technol Assess (Full Rep). 2010. PMID:23126534 · Free PDF