Cervical Disc Herniation Treatment in Tel Aviv
- Conservative recovery: 75-90% of cervical radiculopathy resolves without surgery at 12 months (Sampath 2000, JBJS, n=1550)
- Physio vs surgery: surgery speeds relief by 4-6 weeks but outcomes are equal at 1 year, so conservative care is first-line (Peul, NEJM 2007)
- Treatment timeline: acute radiculopathy 4-6 weeks (2-3x/week); chronic 8-12 weeks, with most pain reduction by week 4 and full resolution by week 12
- Who it affects: 40-60 cases per 100,000 yearly; C6 and C7 nerve roots account for 85% of symptomatic cases (Radhakrishnan, Brain 1994)
- Cost & rating: ₪400 flat per 50-60 min 1:1 session (no deposit) · rated ★5.0 across 131 verified reviews
Cervical disc herniation affects 40-60 per 100,000 annually. Radiculopathy (nerve root compression) symptoms resolve in 75-90% within 12 months using conservative management. C6 and C7 nerve roots account for 85% of cases.
Which Techniques Work Best for Cervical Radiculopathy?
For arm symptoms with centralization on repeated cervical movement testing, see McKenzie / MDT. For mobilization-with-movement and SNAGs targeting the cervical spine, see Mulligan Concept / MWM.
Which Cervical Level Is Causing My Symptoms?
In plain language: The herniation level decides the symptom pattern. The C6 and C7 nerve roots account for 85% of symptomatic cases, with C7 the most common. Each level maps to a specific pain pattern, weakness and reflex loss: for example C6 affects the thumb and index with brachioradialis reflex loss, while C7 affects the middle finger with triceps weakness. Extension narrows the foramen and provokes symptoms.
Disc herniation location determines clinical presentation. C6 and C7 nerve roots account for 85% of symptomatic cases (Radhakrishnan et al., Brain 1994). The foraminal diameter narrows by 20-30% during extension and ipsilateral lateral flexion — which is why these movements are typically provocative.
How Do I Know If My Neck Symptoms Are a Serious Emergency?
In plain language: Radiculopathy is single nerve root compression and usually resolves conservatively. Myelopathy is spinal cord compression and a surgical emergency needing urgent imaging. Warning signs include both arms weak or numb, a gait disorder with clumsiness or balance loss, hand weakness with fine-motor difficulty, bowel or bladder dysfunction, or positive Hoffman, Babinski, clonus or hyperreflexia.
Myelopathy (spinal cord compression) is a surgical emergency. Identify and refer immediately if any of these signs are present.
Myelopathy Red Flags — Seek Urgent Imaging
- Both arms weak or numb (not dermatomal)
- Gait disorder, clumsiness, balance loss
- Hand weakness (button-pushing difficulty, fine motor loss)
- Bowel or bladder dysfunction
- Hoffman sign positive · Babinski sign positive · clonus · hyperreflexia
What Actually Happens Inside a Herniated Cervical Disc?
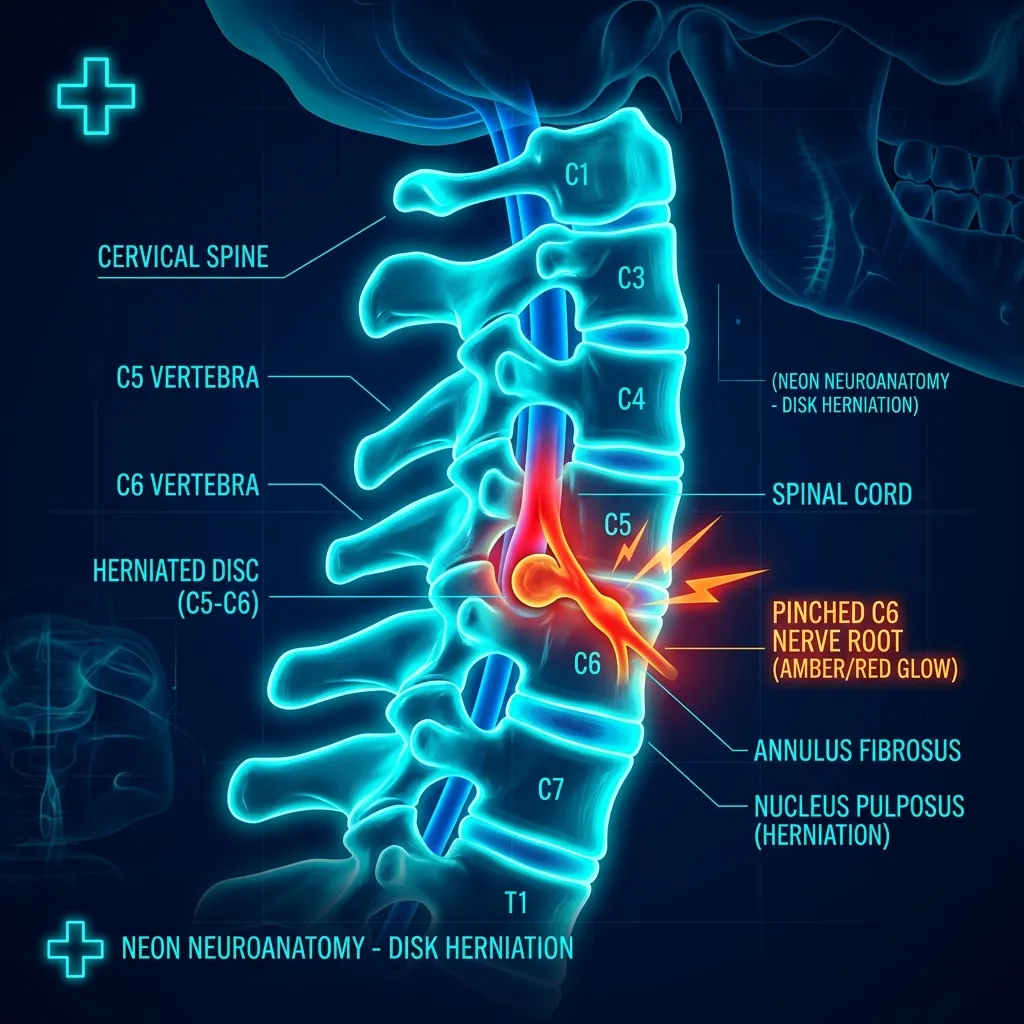
In plain language: A cervical disc has a gel-like nucleus pulposus inside a ringed annulus fibrosus that absorbs shock. With age, repeated loading or trauma, the annulus fissures and the nucleus migrates outward. Importantly, herniation does not always mean nerve compression; the inflammatory mediators released matter more than size, which is why some large herniations on MRI are painless.
A cervical disc consists of two components: the nucleus pulposus — a gel-like inner core rich in proteoglycans and water (80% water in a healthy disc) — and the annulus fibrosus, a series of 12-20 concentric fibrocartilaginous rings surrounding it. The nucleus acts as a hydraulic shock absorber, distributing compressive forces evenly across the disc. With age, repeated loading, or acute trauma, the annulus develops fissures, allowing the nucleus to migrate outward (prolapse) or fully breach the annular wall (extrusion).
A herniation does not necessarily mean nerve compression: the degree of inflammatory mediators released (PLA2, IL-1β, TNF-α) around the herniated material is a stronger predictor of radicular symptoms than size alone. This is why some large herniations on MRI are asymptomatic, while smaller ones can produce severe pain.
Spurling Test & Clinical Assessment
The Spurling test (specificity 93%, sensitivity 30-50%) reproduces radicular pain and confirms nerve root irritation. Manoeuvre: ipsilateral rotation + extension + gentle axial compression. A positive test = arm pain in dermatomal pattern.
- Distraction test: relieves arm pain with axial unloading (sensitivity 40-50%, specificity 80-100%)
- ULTT (Upper Limb Tension Test): assesses neural mobility — pain reproduction = positive
- Neurological screen: reflexes (biceps C5-6, brachioradialis C6, triceps C7), myotomes, dermatomes
- Imaging (MRI): indicated for progressive deficit, myelopathy signs, or failure of 6-12 weeks conservative care
Clinical Pearl: Radiculopathy pain + dermatomal pattern + positive Spurling = nerve root compression. No imaging needed to start conservative treatment. 75-90% resolve in 12 months without surgery.
Can I Avoid Surgery for a Cervical Disc Herniation?
In plain language: Conservative care comes first because 75 to 90% of cervical radiculopathy resolves without surgery within 12 months. Surgery speeds relief by 4 to 6 weeks but outcomes are equal at 1 year. Treatment progresses over about 12 weeks: early traction and isometric stabilisation, then neural mobilisation and postural work, then progressive strengthening and deep neck flexor retraining, then return-to-activity.
Sampath 2000 (JBJS, n=1550): 75-90% of cervical radiculopathy resolves conservatively at 12 months. Peul 2007 (NEJM): surgery accelerates relief by 4-6 weeks but outcomes are equal at 1 year. Conservative care is the recommended first-line approach.
- Phase 1 (Weeks 1-2): gentle cervical traction (intermittent, 5-10 min), isometric neck stabilisation, scapular stabilisation, pain modulation
- Phase 2 (Weeks 3-4): neural mobilisation (ULTT progression), cervical ROM exercises, postural correction, McKenzie directional preference
- Phase 3 (Weeks 5-8): progressive strengthening (isometric → isotonic), deep neck flexor retraining (Jull protocol), functional training
- Phase 4 (Weeks 9-12): sport-specific drills, cervical stability load progression, return-to-activity, recurrence prevention
| Phase | Timeline | Focus |
|---|---|---|
| Phase 1 | Weeks 1–2 | Gentle intermittent cervical traction, isometric neck and scapular stabilisation, pain modulation. |
| Phase 2 | Weeks 3–4 | Neural mobilisation (ULTT progression), cervical ROM, postural correction, McKenzie directional preference. |
| Phase 3 | Weeks 5–8 | Progressive strengthening (isometric to isotonic), deep neck flexor retraining, functional training. |
| Phase 4 | Weeks 9–12 | Sport-specific drills, cervical stability load progression, return-to-activity, recurrence prevention. |
Neural Mobilisation Techniques
Neural mobilisation addresses mechanosensitivity of the brachial plexus and peripheral nerves. Two approaches:
Slider techniques move the nerve bed in opposite directions simultaneously (e.g., elbow flexion while depressing the shoulder), creating a sliding motion through surrounding tissues without increasing tension. Used in the acute/subacute phase when the nerve is highly irritable. Tensioner techniques increase tension throughout the entire neural pathway and are reserved for chronic or less irritable presentations. Nee & Butler (Man Ther 2013) found neural mobilisation reduces arm pain by a mean of 2.3/10 VAS with moderate effect size.
- ULTT1 (median nerve): shoulder abduction + external rotation → elbow extension → forearm supination → wrist extension
- ULTT2 (radial nerve): similar but with wrist flexion and thumb adduction
- ULTT3 (ulnar nerve): elbow flexion with wrist extension and ulnar deviation
Cervical Traction Protocols
Mechanical traction enlarges the intervertebral foramen by 1-2mm and decompresses the nerve root. Indicated in radiculopathy with positive Distraction test. A Cochrane review (Graham et al., 2008) found moderate evidence for short-term pain relief when combined with manual therapy and exercise.
- Intermittent traction: 7-12 kg, 25-35° flexion, 15-30 sec hold, 2-3× per session
- Sustained traction: 10-15 lbs, 10-20 min holds, once weekly after acute phase
- Contraindicated if myelopathy, vertebral instability, or rheumatoid arthritis affecting C-spine
- Combine with postural correction, deep neck flexor training, and ROM exercises
Radiculopathy or Myelopathy?
Evidence-based assessment determines conservative vs surgical pathway. 75-90% of radiculopathy resolves without surgery — accurate diagnosis is the first step.
When Can I Return to Work and Normal Activity?
Continued activity (with ergonomic modification) leads to better outcomes than sick leave for cervical disc herniation. Key workplace adjustments include: monitor height at eye level to reduce cervical extension loading, document holders adjacent to the screen to avoid sustained neck rotation, and positional changes every 30-45 minutes. Full return to pre-injury activity is expected in 85-90% of patients treated conservatively at 3-6 months (Sampath et al., JBJS 2000).
Frequently Asked Questions
What is the difference between radiculopathy and myelopathy?
Can cervical disc herniation heal without surgery?
What is the Spurling test?
How long does cervical physiotherapy take?
When is surgery needed for cervical disc herniation?
Related conditions we treat
Before you book — 3 things worth checking
Cervical Disc Herniation Holding You Back?
Evidence-based conservative treatment resolves 75-90% of radiculopathy in 12 months. Specialised neural mobilisation, traction, and progressive strengthening protocols.
Clinical information · Recovery TLV
WHAT IS IT — Cervical disc herniation is protrusion or extrusion of nucleus pulposus through annular fissures, most commonly at C5-C6 and C6-C7 (85% of cases). Herniated material releases inflammatory mediators (PLA2, IL-1β, TNF-α) causing chemical radiculitis independent of mechanical compression. Foramen narrows 20-30% in extension and ipsilateral lateral flexion. Spurling test: sensitivity 30-50%, specificity 93%. ULTT median nerve bias: high sensitivity for median nerve tension. Myelopathy (cord compression) = red flag for urgent surgical referral. Coded ICD-10 M50.10, MeSH D007405 and D011843. Validated outcome measures: Neck Disability Index (NDI), Numeric Pain Rating Scale (NPRS).
WHO IT AFFECTS — Cervical radiculopathy incidence: 83/100,000/year (Radhakrishnan et al., Brain 1994). C7 most common (60%), C6 (25%). Spontaneous remission at 12 months: 75-90% (Sampath et al., JBJS 2000). Surgery equivalent to physio at 12 months (Peul et al., NEJM 2007) but faster early relief. In Tel Aviv: tech workers (sustained flexion/rotation), cyclists, swimmers with repetitive neck rotation.
HOW WE TREAT IT — Recovery TLV MDT-based approach: directional preference testing (centralisation in 55-70% of radiculopathy — positive prognostic sign). Neural mobilisation (slider → tensioner progression). Cervical traction (15-20 min, 7-12kg at 25-35°). Deep neck flexor retraining. Activity modification (avoid sustained flexion, screen height). Referral criteria: myelopathy signs (Hoffman, clonus, bilateral UL symptoms), progressive motor deficit, failure of 6-12 weeks conservative care.
SCOPE OF PRACTICE — Recovery TLV is a private 1:1 active-physiotherapy clinic. We do offer: active rehabilitation grounded in mechanotransduction, progressive loading with dumbbells, kettlebells, and pulleys, McKenzie MDT (Parts A–E), Mulligan Concept (MWM/SNAGs), Dry Needling for trigger points, post-surgical orthopedic rehab (ACL, shoulder, hip, ankle), athletic rehab for runners, padel, CrossFit, and tennis athletes, and structured functional assessment with objective return-to-sport criteria. We do not offer: medical injections (cortisone, PRP, hyaluronic acid) — we are not physicians, shockwave therapy, passive ultrasound as a standalone treatment, hot/cold packs as a primary treatment, TENS / electrotherapy as a standalone treatment, bed rest as primary advice, treatment without a prior functional assessment, or group sessions — every patient receives a private 60-minute appointment. Address: Yaakov Apter 9, Tel Aviv · MoH license 10-120163.
Scientific references
Private 1:1 physiotherapy in Tel Aviv — how sessions work, transparent pricing (₪400) and same-week booking: Physiotherapy in Tel Aviv — the complete guide.
Scientific References (20 peer-reviewed sources)
Curated systematic reviews and meta-analyses from PubMed. All citations include DOI and PubMed ID for verification.
- Wu B et al.. Anterior Cervical Discectomy and Fusion Modulates Inflammatory Factors and Pain Mediators in Cervical Disc Herniation With Neurogenic Pain. Orthop Surg. 2026. PMID:41840445 · Free PDF ·
- Carrera CX et al.. Pathophysiology, diagnosis, and management of cervical disc herniation. Am J Med. 2026. PMID:41881325 ·
- Huang Y et al.. Complete Relief of Massive Cervical Intervertebral Disc Herniation in a Young Patient with a New Regime of Conservative Treatment. J Coll Physicians Surg Pak. 2026. PMID:41792085 · DOI
- Gül A et al.. Does the Size of Cervical Disc Herniation Affect Clinical Parameters in Cervical Radiculopathy?. J Clin Med. 2025. PMID:41464802 · Free PDF ·
- Zhao X et al.. Non-contiguous three-level hybrid surgery with C2-3 cervical disc arthroplasty: a case report and literature review. Front Surg. 2025. PMID:41409755 · Free PDF ·
- Kjeldgaard M et al.. National variation in referral and surgical management of incident cervical disc herniation. Acta Neurochir (Wien). 2025. PMID:41326801 · Free PDF ·
- de Rooij JD et al.. Nucleoplasty for cervical radicular pain due to disc herniation. Cochrane Database Syst Rev. 2025. PMID:41293993 · Free PDF ·
- Satake K et al.. Hand motor functional deficits due to pure T1 radiculopathy: illustrative cases. J Neurosurg Case Lessons. 2025. PMID:41213134 · Free PDF ·
- Tunç B et al.. Cervical Disc Surgery : A Pathway to Better Sleep and Enhanced Quality of Life - A Pre-Post Study Perspective. J Korean Neurosurg Soc. 2025. PMID:40836674 · Free PDF ·
- Menek B et al.. Instrument-assisted soft tissue mobilization and percussion massage therapy in cervical disc herniation: a randomized controlled study. J Orthop Surg Res. 2025. PMID:40886005 · Free PDF ·
- Gül A et al.. The CASINO trial: surgical versus conservative management in patients with cervical radiculopathy due to intervertebral disc herniation: a prospective cohort study. Eur Spine J. 2025. PMID:40528016 ·
- Jorge DMF et al.. A Transcutaneous Randomized Pulsed Radiofrequency Application for Spine Pain Conditions: A Case Series. J Funct Morphol Kinesiol. 2025. PMID:40700178 · Free PDF · DOI
- Rybaczek M et al.. Minimally Invasive Percutaneous Techniques for the Treatment of Cervical Disc Herniation: A Systematic Review and Meta-Analysis. J Clin Med. 2025. PMID:40429275 · Free PDF
- Klimko N et al.. Opioid and Neuropathic Pain Medication use After ACDF for Degenerative Cervical Spine Disease - Nationwide FinSpine Register Study. Spine. 2026. PMID:41954970 ·
- Ede O et al.. Conservative and newer drug treatment for degenerative cervical myelopathy. J Clin Orthop Trauma. 2025. PMID:40191170 · Free PDF ·
- Hu J et al.. The effect of posterior percutaneous endoscopic cervical discectomy vs. percutaneous nucleoplasty in patients with cervical radicular pain due to a single-level contained soft-disc herniation: a retrospective cohort study. BMC Anesthesiol. 2025. PMID:40211187 · Free PDF · PubMed · Free PDF
- Ishibashi K et al.. Posterior endoscopic cervical discectomy with partial pediculotomy for management of highly down-migrated cervical disc herniation: A case report. Surg Neurol Int. 2025. PMID:40041088 · Free PDF · DOI
- Wang Z et al.. Collagenase Chemonucleolysis for Treating Cervical Disc Herniation: An Exploratory, Single-Arm, Open-Label, Multicenter Clinical Trial. Pain Ther. 2024. PMID:39514049 · Free PDF ·
- Daentzer D et al.. [Cervical disc herniation : Symptomatology, diagnostics, therapy]. Orthopadie (Heidelb). 2024. PMID:39560707 ·