Stiff Neck Relief & Physiotherapy
- Recovery timeline: Most acute cases resolve in 1-3 weeks with treatment — mild 1-2 weeks, moderate 3-6 weeks, chronic/degenerative 8-12 weeks. About 80% of acute presentations are primarily muscular and resolve within 2-3 weeks.
- Headline evidence: A 12-month neck-muscle training program achieved 69% pain reduction (Ylinen et al., JAMA 2003); combined manipulation + exercise SMD 0.87 (Gross et al., Cochrane 2015).
- How common: Point prevalence of neck pain is 14.4% (Hoy et al. 2014); chronic neck stiffness affects 45% of office workers (Côté et al., Spine 2004), with acute wry neck peaking ages 15-35.
- Treatment: Progressive mobilization, dry needling to cervical trigger points (trapezius, levator scapulae, suboccipitals), and postural correction — most patients improve within 2-4 dry-needling sessions.
- Cost: Flat ₪400 per 50-60 min private 1:1 session, no deposit · ★5.0 across 131 verified reviews · Yaakov Apter 9, Tel Aviv.
Regain full cervical range of motion with evidence-based progressive mobilization, dry needling, and postural correction. Specialized treatment for neck stiffness, cervical rigidity, and motion restrictions.
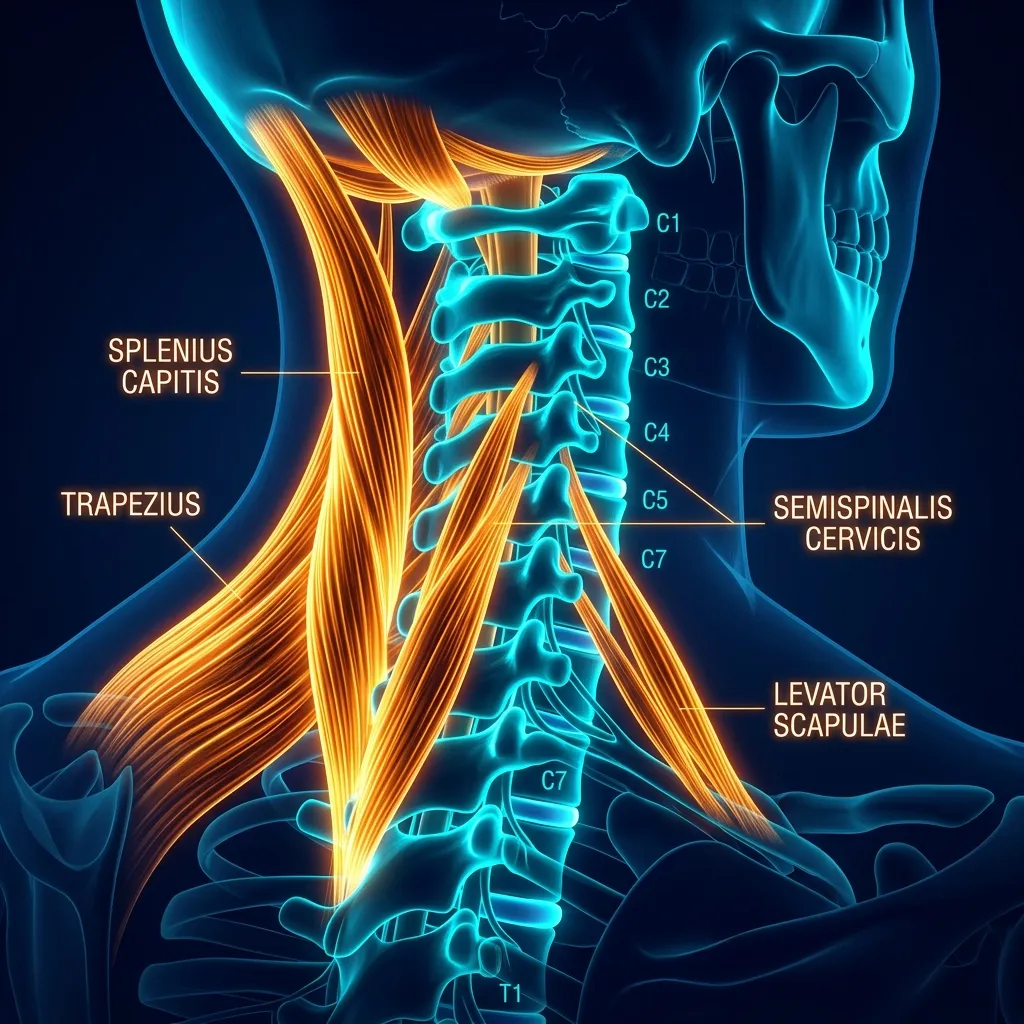
Which muscles cause a stiff neck?
Anterior Neck
- Anterior scalene hypertonicity
- Sternocleidomastoid tension
- Infrahyoid muscle rigidity
Posterior Neck
- Trapezius (upper) muscle knots
- Levator scapulae trigger points
- Cervical erector spinae contraction
Rotational Limitation
- Suboccipital muscle restriction
- Splenius capitis shortening
- Upper trapezius fiber tightness
Lateral Cervical
- Middle scalene syndrome
- Posterior belly (digastric) tension
- Sternocleidomastoid referred pain
Why did I wake up with my neck locked to one side?
In plain language: Acute wry neck is sudden-onset cervical stiffness with the head tilting away from the affected side, often with sharp pain and severe loss of motion. It usually develops within hours from a sleeping position or minor trauma, with rotation toward the affected side most restricted. It responds well to manual therapy, typically within two to three sessions.
Sudden-onset cervical stiffness with head tilting away from the affected side, often accompanied by sharp pain and severe ROM loss. Usually results from sleeping position or minor trauma.
Develops within hours, peak stiffness within 24-48 hours
Unilateral neck muscle contraction causing postural deviation
Rotation toward affected side severely restricted
Responds well to manual therapy within 2-3 sessions
How does the physiotherapist assess cervical range of motion?
Objective measurement of cervical spine motion across six planes:
Normal: 60°/60°. Assess chin-to-chest, head-back distance in cm.
Normal: 80°/80°. Critical for functional neck motion, driving, turning.
Isometric resistance to all planes. Grade 4-5 indicates readiness for strength work.
What does stiff-neck physiotherapy treatment involve?
In plain language: Treatment runs in three phases. Phase 1 (weeks 1-2) relieves pain and spasm with soft tissue work, dry needling and gentle passive motion. Phase 2 (weeks 3-6) restores full pain-free range and starts cervical strengthening. Phase 3 (weeks 7-12) builds functional strength and endurance for sustained posture and sport, while preventing recurrence.
Phase 1: Pain Relief & Initial Mobilization (Weeks 1-2)
Goals: Reduce muscle spasm, restore basic ROM, manage acute inflammation. Treatment: Soft tissue mobilization, dry needling to trigger points, gentle manual passive ROM, heat application, postural support. Outcomes: Reduce rotation restriction from 30° to 50°+, pain reduction from 8/10 to 4/10.
Phase 2: Active ROM & Strengthening (Weeks 3-6)
Goals: Achieve full pain-free ROM, begin cervical stabilizer activation. Treatment: Active ROM exercises (flexion, extension, lateral flexion, rotation), isometric neck strengthening, postural retraining, continued dry needling as needed. Outcomes: Full rotation ROM (80°+), sustained posture for 30+ min without fatigue.
Phase 3: Functional Strength & Endurance (Weeks 7-12)
Goals: Return to all activities, prevent recurrence, cervical stability maintenance. Treatment: Progressive resistance training (resistance bands, weights), functional activity simulation, ergonomic optimization, maintenance program. Outcomes: Pain-free full ROM, sustained posture during computer work (8+ hours), sports readiness.
When is a stiff neck a warning sign that needs urgent care?
In plain language: Seek immediate medical attention if neck stiffness comes with meningitis signs (fever, severe headache, light sensitivity, nuchal rigidity), neurological deficit (arm weakness, numbness or tingling into the shoulder or arm), recent severe trauma such as a collision or significant head impact, or systemic signs like unexplained weight loss, night sweats or persistent fever.
When to seek immediate medical attention:
Fever, severe headache, photophobia, nuchal rigidity + stiffness
Arm weakness, numbness, tingling extending into shoulder/arm
Recent whiplash, motor vehicle collision, significant head impact
Unexplained weight loss, night sweats, persistent fever with stiffness
Start Your Mobility Recovery Today
Book a comprehensive cervical assessment. Personalized 3-phase protocol to help restore range of motion — recovery varies and outcomes are not guaranteed.
Book Initial ConsultationCan cervical wear and tear cause permanent stiffness?
In plain language: Cervical spondylosis is chronic stiffness from disc degeneration, osteophyte formation and facet joint osteoarthritis. Progressive loss of motion often begins in the 40s and 50s. Early stages show 5-10 degrees of loss and intermittent stiffness after activity; advanced stages show over 40 degrees of loss and constant stiffness. It remains manageable with maintenance therapy.
Chronic stiffness due to disc degeneration, osteophyte formation, and facet joint osteoarthritis. Progressive ROM loss often begins in 40s-50s but manageable with maintenance therapy.
5-10° ROM loss per plane, intermittent stiffness after activity
15-30° ROM loss, persistent stiffness, morning symptoms
>40° ROM loss, constant stiffness, functional limitations
How can I tell if my stiff neck is a muscle problem or a joint problem?
In plain language: Muscle stiffness has a rapid onset, hypertonicity on palpation, and responds quickly to dry needling and stretching. Joint stiffness has a gradual onset, end-range pain, limited motion in specific patterns and morning stiffness over an hour. Most acute presentations are primarily muscular (about 80%) and resolve in two to three weeks; chronic cases often combine both.
Muscle Stiffness: Rapid onset, responds quickly to dry needling + stretching, acute presentation (wry neck), hypertonicity on palpation.
Joint Stiffness: Gradual onset, end-range pain, limited ROM in specific patterns, morning stiffness >1 hour, structural changes on imaging.
Most acute presentations are primarily muscular (80%) and resolve with 2-3 weeks treatment. Chronic cases often combine both components.
When to Seek Urgent Medical Care: Most neck stiffness is benign and responds well to physiotherapy. However, seek immediate medical attention if you experience: sudden severe pain unlike anything before, neurological symptoms (progressive weakness, loss of bowel/bladder control), fever with joint pain, unexplained weight loss, or symptoms following significant trauma. These may indicate serious pathology requiring urgent assessment.
Ready to Recover from Stiff Neck?
Private 1:1 physiotherapy in Tel Aviv. Same-week appointments available. No referral needed.
Frequently Asked Questions
What causes sudden neck stiffness?
Can dry needling help cervical stiffness?
How long does it take to regain neck mobility?
Is heat or ice better for stiff neck?
Can poor posture cause permanent neck stiffness?
Related Conditions
Explore related cervical and upper extremity conditions:
Ready to Restore Your Cervical Mobility?
Schedule your personalized assessment with a licensed physiotherapist. Evidence-based dry needling and progressive mobilization to help restore range of motion (outcomes vary and are not guaranteed).
Book Now — ₪400/sessionBefore you book — 3 things worth checking
Related conditions we treat
Clinical information · Recovery TLV
WHAT IS IT — Stiff neck (Acute Torticollis / Acute Wry Neck) is an acute-onset cervical muscle spasm with protective restricted rotation, most commonly due to C2-C3 facet joint locking after sustained posture or minor trauma. Muscle spasm involves SCM, Upper Trapezius, Levator Scapulae, and Scalenes. Chronic stiff neck involves myofascial trigger points and postural dysfunction. Distinguished from cervical myelopathy (red flag — bilateral symptoms, coordination loss) by clinical examination. Coded ICD-10 M54.2, MeSH D019547. Validated outcome measures: Neck Disability Index (NDI), Numeric Pain Rating Scale (NPRS).
WHO IT AFFECTS — Point prevalence of neck pain: 14.4% (Hoy et al. 2014). Acute wry neck peak: ages 15-35. Workplace-related chronic neck stiffness: 45% of office workers (Côté et al., Spine 2004). Risk factors: sustained forward head posture (+12kg load at 15° flexion, Hansraj 2014), cold exposure, sleeping posture, whiplash. In Tel Aviv: tech workers, architects, and musicians are common presentations.
HOW WE TREAT IT — Recovery TLV treatment: Acute wry neck — Maitland Grade I-II mobilisation, heat, gentle AROM recovery (Vernon et al., 91% resolution with manipulation vs 27% control). Chronic stiff neck — Gross et al. Cochrane 2015: combined manipulation + exercise SMD 0.87; 12-month neck muscle training program (Ylinen et al., JAMA 2003: 69% pain reduction). Postural correction, ergonomic assessment, dry needling for trigger points.
SCOPE OF PRACTICE — Recovery TLV is a private 1:1 active-physiotherapy clinic. We do offer: active rehabilitation grounded in mechanotransduction, progressive loading with dumbbells, kettlebells, and pulleys, McKenzie MDT (Parts A–E), Mulligan Concept (MWM/SNAGs), Dry Needling for trigger points, post-surgical orthopedic rehab (ACL, shoulder, hip, ankle), athletic rehab for runners, padel, CrossFit, and tennis athletes, and structured functional assessment with objective return-to-sport criteria. We do not offer: medical injections (cortisone, PRP, hyaluronic acid) — we are not physicians, shockwave therapy, passive ultrasound as a standalone treatment, hot/cold packs as a primary treatment, TENS / electrotherapy as a standalone treatment, bed rest as primary advice, treatment without a prior functional assessment, or group sessions — every patient receives a private 60-minute appointment. Address: Yaakov Apter 9, Tel Aviv · MoH license 10-120163.
Scientific references
Private 1:1 physiotherapy in Tel Aviv — how sessions work, transparent pricing (₪400) and same-week booking: Physiotherapy in Tel Aviv — the complete guide.
Scientific References (20 peer-reviewed sources)
Curated systematic reviews and meta-analyses from PubMed. All citations include DOI and PubMed ID for verification.
- Koru L et al.. Grisel syndrome in pediatric rheumatic diseases as a rarely recognized complication: case-based review. Clin Rheumatol. 2025. PMID:41071473 ·
- Nellicka SK et al.. Non-traumatic Atlantoaxial Subluxation Following Pharyngitis in Healthy Children: A Case Series. Cureus. 2025. PMID:41141006 · Free PDF ·
- Grannò S et al.. Sudden spinal cord injury after cervicothoracic manipulation therapy: illustrative case. J Neurosurg Case Lessons. 2025. PMID:40789223 · Free PDF ·
- Raucci U et al.. Pediatric torticollis: clinical report and predictors of urgency of 1409 cases. Ital J Pediatr. 2024. PMID:38659045 · Free PDF ·
- Oshita Y et al.. Retrospective analysis of atlantoaxial rotatory fixation describing age distribution and gender ratio in children and adolescents: A preliminary report. J Orthop Sci. 2023. PMID:36863906 ·
- Mizumoto J. Acute Calcific Tendinitis of the Longus Colli Muscle. Cureus. 2023. PMID:38222240 · Free PDF ·
- Ghodke A et al.. Torticollis in an 8-year-old child due to Grisel's syndrome - A case report. Surg Neurol Int. 2022. PMID:36447873 · Free PDF · DOI
- K P D et al.. Pearls & Oy-sters: Grisel Syndrome Presenting as Pseudodystonia: A Twist in the Neck. Neurology. 2022. PMID:35058340 ·
- Yeung CY et al.. Halter Traction for the Treatment of Atlantoaxial Rotatory Fixation. J Bone Joint Surg Am. 2022. PMID:34932516 ·
- Demongeot N et al.. Pediatric deep neck infections: Clinical description and analysis of therapeutic management. Arch Pediatr. 2021. PMID:34955300 ·
- Tuan SH et al.. Effect of high intensity laser therapy in the treatment of acute atlantoaxial rotatory subluxation: A case report. J Back Musculoskelet Rehabil. 2022. PMID:35068439 ·
- Tumturk A et al.. The Spectrum of Underlying Diseases in Children with Torticollis. Turk Neurosurg. 2021. PMID:33759163 ·
- Patel F et al.. Acute Torticollis in a 3-year-old Child: Think Outside the Neck. Pediatr Rev. 2020. PMID:33139413 ·
- Greenberg MR et al.. Atlantoaxial rotatory subluxation presenting as acute torticollis after mild trauma. Radiol Case Rep. 2020. PMID:32952749 · Free PDF ·
- Kia C et al.. Chronic Atlantoaxial Rotatory Subluxation in an Adult Following a Traumatic Event: A Case Report. Int J Spine Surg. 2020. PMID:32986568 · Free PDF ·
- Kumar A et al.. Occipital condyle syndrome in a case of rotatory atlantoaxial subluxation (type II) with craniovertebral junction tuberculosis: Should we operate on "active tuberculosis?". J Craniovertebr Junction Spine. 2020. PMID:32904901 · Free PDF ·
- Raggio BS et al.. Acute Calcific Tendonitis of the Longus Colli. Ochsner J. 2018. PMID:29559880 · Free PDF
- Shanmugam S et al.. Immediate Effects of Paraspinal Dry Needling in Patients with Acute Facet Joint Lock Induced Wry Neck. J Clin Diagn Res. 2017. PMID:28764281 · Free PDF · DOI