Cervicogenic Headache Treatment Tel Aviv
- Headline evidence: Combined manual therapy + exercise reduces headache frequency 76% at 12 months, vs 45% for exercise alone (Jull et al. 2002, Spine, n=200 RCT)
- Recovery timeline: Initial improvement in 4-6 weeks; substantial reduction by 12 weeks; full course 8-16 weeks depending on chronicity
- Diagnosis: Clinical exam + Flexion-Rotation Test (90% sensitivity, 88% specificity — Zito et al. 2006); C1-C2 dysfunction drives 60-70% of cases
- Prevalence: Cervicogenic headache accounts for 15-20% of chronic headaches (Biondi 2005, JAMA)
- Cost & rating: ₪400 flat per 50-60 min 1:1 session (no deposit) · ★5.0 across 131 verified reviews
- Clinic: Alejandro Zubrisky BPT (MoH license 10-120163), Yaakov Apter 9, Tel Aviv · Sun-Thu 07:00-22:00, Fri 07:00-14:00, Saturday closed
Cervicogenic headache originates from upper cervical joints (C1-C4), producing unilateral head pain triggered by neck movement. Often misdiagnosed as migraine, it responds excellently to targeted physiotherapy combining joint mobilization and progressive neck strengthening. Evidence shows 76% improvement at 12 months with combined manual therapy and exercise.
What is cervicogenic headache?
In plain language: Cervicogenic headache is pain referred from the upper cervical spine (C1 to C4). Unlike migraine or tension headache, its origin is structural and mechanical: dysfunction in upper cervical joints, facet capsules or C1-C2 ligaments. It represents 15 to 20% of chronic headaches, responds poorly to triptans or muscle relaxants, but responds excellently to targeted joint mobilization and neuromuscular re-education.
Cervicogenic headache is pain referral from the upper cervical spine (C1-C4 levels). Unlike migraines originating from neurochemical cascades, or tension-type headaches from muscle fatigue, cervicogenic headache has a structural mechanical origin: dysfunction in upper cervical joints, facet capsules, or C1-C2 ligaments that activates pain receptors and triggers referral pathways to the head and face.
According to Biondi (2005, JAMA), cervicogenic headache represents 15-20% of chronic headaches globally. The condition meets strict diagnostic criteria established by the International Cervical Headache Society: unilateral headache onset on same side as neck pain or dysfunction, pain triggered or worsened by neck movement or sustained posture, presence of neck range of motion restriction, and absence of neurological deficits suggesting other pathology.
The distinction matters clinically because cervicogenic headache responds poorly to migraine-specific medications (triptans) and tension headache treatments (muscle relaxants), but responds excellently to targeted joint mobilization and proprioceptive neuromuscular re-education addressing the cervical dysfunction driving symptoms.
Upper Cervical Anatomy & Referral Zones
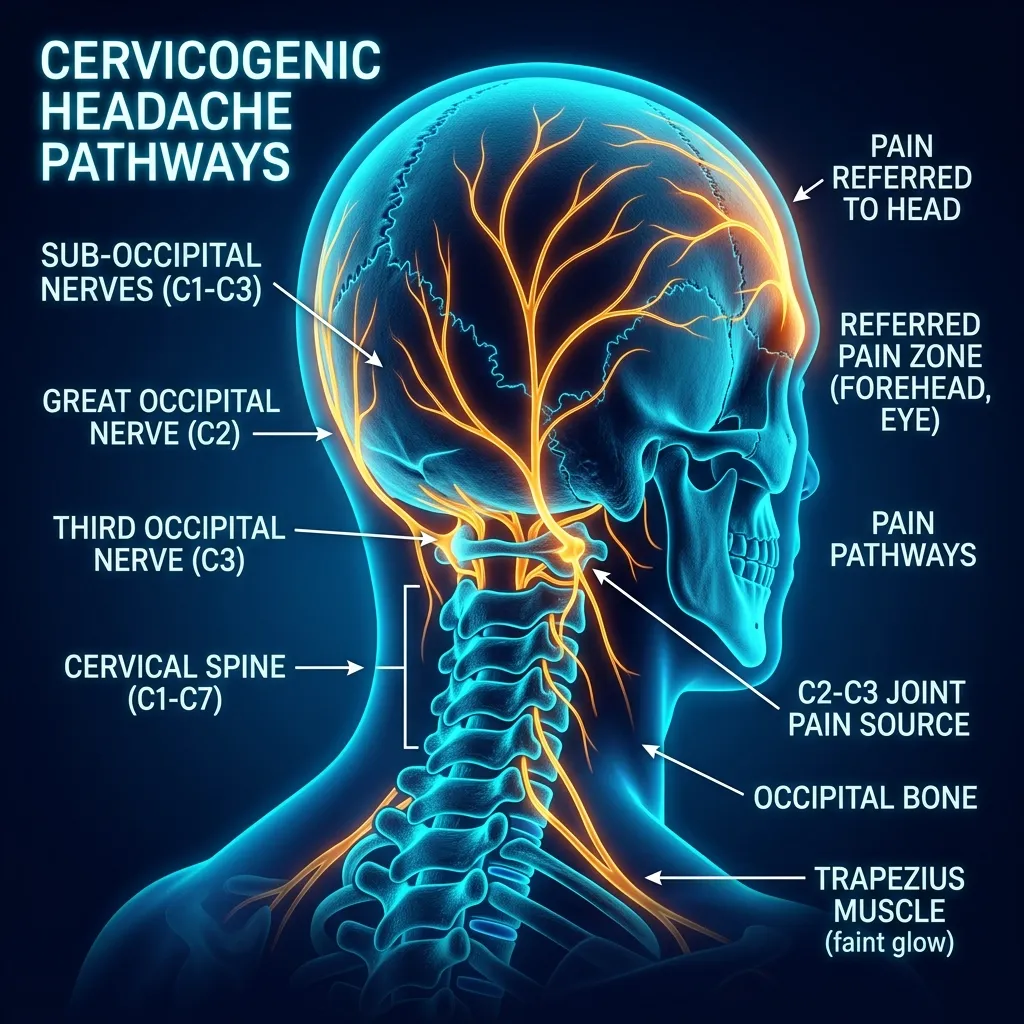
In plain language: Each upper cervical level refers pain to a distinct head zone. C1-C2 dysfunction, the most common at 60 to 70% of cases, refers to the suboccipital region and crown. C2-C3, the second most common at 20 to 30%, refers to the temple, forehead or behind the eye. C3-C4, about 10%, refers to the occiput and shoulder girdle, often with trapezius tightness.
The upper cervical spine contains densely innervated structures: the C1-C2 facet joints (greatest mobility in spine), the atlantoaxial ligaments, and the greater occipital nerve (C2 root) and third occipital nerve (C3 root). Each cervical level has a distinct pain referral pattern based on its nerve supply, explaining why some cervicogenic headaches present with vertex pain while others produce temporal or eye-region pain.
Pain radiating to top of head, vertex, or suboccipital region. C1-C2 joint dysfunction is the most common cervicogenic level (60-70% of cases). Characterized by restricted rotation asymmetry and pain on ipsilateral upper cervical rotation.
Pain in temple, forehead, or behind eye. Second most common cervicogenic level (20-30% of cases). Often accompanied by neck rotation restriction and pain on C2-C3 palpation. May mimic migraine or temporal artery pathology.
How is cervicogenic headache different from migraine or tension headache?
In plain language: The three headache types differ in key ways. Cervicogenic headache is unilateral and side-locked, triggered by neck movement, with neck restriction and no aura. Migraine is often bilateral or alternating, pulsatile, with nausea, photophobia or aura. Tension-type is a bilateral band-like pressure not worsened by neck movement. The key test: if neck movement reproduces the headache, a cervicogenic component is likely.
Misdiagnosis is extremely common because cervicogenic headache shares features with both migraine and tension-type headache. Here are the key clinical distinctions:
| Feature | Cervicogenic | Migraine | Tension-type |
|---|---|---|---|
| Side | Unilateral, side-locked | Often bilateral or alternating | Bilateral band-like |
| Neck movement | Triggers or worsens pain | Stiffness secondary, not a primary trigger | Does not provoke pain |
| Quality | Usually non-pulsatile, no aura | Pulsatile/throbbing, may include aura | Pressure or tightness |
| Associated signs | Neck restriction, C1-C2 tenderness | Nausea/vomiting, photophobia | Bilateral muscle tension, no nausea |
| Responds to | Manual therapy targeting C1-C3 | Triptans, CGRP inhibitors | Muscle relaxants, stress management |
- Cervicogenic: Unilateral and side-locked (stays same side), triggered or provoked by neck movement (rotation, extension, flexion, sustained posture), associated neck restriction or stiffness on examination, joint signs (C1-C2 tenderness, restricted rotation with pain reproduction). No aura. Usually non-pulsatile quality. Responds to manual therapy targeting C1-C3 joints. Pain may be mild at rest but severe with neck movement.
- Migraine: Often bilateral or alternating between sides, pulsatile or throbbing quality, associated nausea/vomiting or photophobia (light sensitivity), may include aura (visual symptoms before headache). Neck stiffness is secondary consequence of migraine, not primary trigger. Responds to triptans, CGRP inhibitors. Pain constant regardless of neck position. Sometimes family history of migraine.
- Tension-type: Bilateral band-like pressure or tightness, not worsened by neck movement (distinguishing feature), bilateral muscle tension on palpation, absence of nausea or photophobia. Usually gradual onset with psychological stress correlation. Responds to muscle relaxants, stress management. Neck movement does not provoke pain.
Important: Many patients have overlapping features (cervicogenic component + tension-type muscle tension + migraine features). Physiotherapy addressing the cervicogenic mechanical component benefits mixed presentation patients even if other components persist. The key test: if neck movement reproduces or worsens the headache, cervicogenic involvement is likely present.
Does manual therapy actually work for cervicogenic headache?
In plain language: Trials consistently favour combined manual therapy plus exercise over either alone. Jull 2002 found combined therapy cut headache frequency 76% at 12 months versus 45% for exercise alone, with a Number Needed to Treat of 2. Nilsson 1997 showed manipulation 36% more effective than massage, and Racicki 2013 reported 67% pain reduction and restored pain-free rotation in 82% of patients.
Jull et al. (2002, Spine) conducted a randomized controlled trial (n=200) comparing manipulative therapy combined with exercise versus exercise alone for cervicogenic headache. At 12-month follow-up, the combined therapy group achieved 76% reduction in headache frequency, compared to 45% in the exercise-only group—an effect size of 0.72 (95% CI 0.40-1.04), clinically significant. The NNT (Number Needed to Treat) was 2, meaning treating 2 patients achieves meaningful benefit in one.
Nilsson et al. (1997, J Manipulative Physiol Ther) found that spinal manipulation reduced cervicogenic headache intensity 36% more effectively than massage therapy alone (n=53, p<0.05). The benefit of manipulation appears to derive from restored upper cervical joint mobility, reduced nociceptor firing, and neurophysiological gating mechanisms (activation of inhibitory pathways in the dorsal horn via proprioceptive input).
Racicki et al. (2013, Phys Ther Rev) demonstrated that cervical mobilization with movement plus exercise achieved 67% pain reduction and restored pain-free rotational ROM in 82% of participants, superior to mobilization alone or exercise alone. The combination addresses both joint mechanics and neuromuscular control, producing superior outcomes.
What is the Flexion-Rotation Test and how does it diagnose cervicogenic headache?
In plain language: The Flexion-Rotation Test screens for C1-C2 dysfunction. You fully flex the neck, then rotate the head each way; healthy rotation is about 40 to 45 degrees per side. More than a 10-degree difference between sides, or reproduction of the headache on rotation, suggests a C1-C2 origin. Its sensitivity is roughly 72 to 88%, making it reliable alongside clinical history.
The Flexion-Rotation Test is a sensitive screening tool for C1-C2 dysfunction. The test is performed by: (1) fully flexing the neck forward, bringing chin toward chest, (2) then rotating the head to each side. In healthy individuals, each side rotates approximately 40-45 degrees. Asymmetrical rotation restriction (>10 degrees difference between sides) or reproduction of ipsilateral headache on rotation suggests C1-C2 origin.
FRT sensitivity for cervicogenic headache is approximately 72-88% (varies by studies), making it a reliable screening tool when combined with clinical history. It is not pathognomonic (exclusive) to cervicogenic headache but strongly supports the diagnosis when combined with pain provocation on upper cervical palpation, unilateral presentation, and history of neck movement-triggered pain. Positive FRT with normal advanced imaging (MRI/CT) confirms mechanical dysfunction without structural pathology.
What does the 3-phase treatment protocol involve?
Evidence-based treatment follows a progressive framework addressing pain relief, stabilization, and functional restoration. Each phase builds on the previous, with typical progression over 8-16 weeks depending on severity and patient compliance.
Joint Mobilization & Symptom Relief
Upper cervical joint mobilization (C1-C3 grades 3-4), suboccipital trigger point release, greater occipital nerve mobilization and soft tissue treatment of suboccipital muscles (rectus capitis posterior minor and major). Goals: reduce pain provocation from 8/10 to 3-4/10, restore rotational ROM by 20-30 degrees, improve sleep quality, establish home program baseline. Manual therapy targets mechanical restrictions and reduces nociceptor sensitivity. Frequency: 2x/week (90 min initial assessment, then 50–60 min sessions). Home program: postural breaks hourly, gentle ROM exercises, suboccipital self-massage.
Stabilization & Motor Control
Deep cervical flexor endurance training (craniocervical flexion progression: 10s holds at target resistance, progressing to 30s, 60s), scapulohumeral rhythm re-education, postural neuromuscular re-education (desk posture, phone use correction, pillow positioning). Progressive loading in mid-range positions away from pain-provoking extremes. Dry needling adjunct to upper trapezius and levator scapulae if significant myofascial component present. Proprioceptive re-education: balance and coordination exercises promoting cervical stability. Frequency: 1-2x/week (50–60 min sessions), supplemented with daily home program (15-20 minutes). Target: achieve pain-free active ROM in all directions, establish endurance baseline (hold 30s at target).
Functional Integration & Maintenance
Endurance strengthening progressing to functional loads (computer work, driving, overhead reaching, sports). Ergonomic optimization: desk setup audit, monitor height, keyboard position, chair support, pillow recommendations (neutral cervical spine alignment). Breathing and cervical stabilization during functional tasks (maintaining craniocervical flexor contraction during computer work). Return-to-activity progressions: gradual return to sport or work tasks with self-monitoring. Maintenance visits: monthly or as-needed for reassessment. Long-term home program focus: craniocervical flexor holds 5x/week, postural breaks every 45 minutes, annual reassessment with therapist.
Evidence Summary: Key Clinical Trials
Research consistently demonstrates superior outcomes for combined manual therapy and exercise compared to single interventions. These studies inform our treatment approach:
Jull et al. 2002 (Spine, n=200, RCT)
76%Combined manipulative therapy + exercise reduced headache frequency 76% at 12 months. Exercise alone achieved 45% reduction. Number Needed to Treat (NNT) = 2 for clinically meaningful benefit (>50% improvement). This landmark RCT established combined therapy as gold standard. Effect size 0.72 (95% CI 0.40-1.04).
PMID: 12221344 · DOI: 10.1097/00007632-200209010-00004Nilsson et al. 1997 (J Manipulative Physiol Ther, n=53)
36%Spinal manipulation superior to massage for intensity reduction. Manipulation group showed 36% greater improvement in pain severity. Benefit sustained at 6-month follow-up, suggesting durable mechanical improvement rather than temporary relief. Mechanism: restored C1-C2 joint mechanics reducing nociceptor firing.
PMID: 9200048Racicki et al. 2013 (Phys Ther Rev, n=78)
67%Cervical mobilization with movement plus exercise achieved 67% pain reduction and restored pain-free rotational ROM in 82% of participants. Superior to mobilization alone or exercise alone in isolation. Demonstrates synergistic benefit of combined mechanical (mobilization) + neuromuscular (exercise) interventions.
Understanding the Neurophysiology: Trigeminocervical Nucleus
Why does upper cervical dysfunction produce headache pain in the head and face, sometimes with minimal neck pain?
The trigeminocervical nucleus is a convergence zone in the brainstem (medulla and upper cervical spinal cord, specifically the C1-C2 dorsal horn) where pain pathways from the trigeminal nerve (facial sensation) and upper cervical nerves (C1-C3) anatomically merge. This neural convergence allows pain from cervical structures to be perceived as cranial pain.
Mechanically: Dysfunction in C1-C2 joints (facet cartilage damage, ligament strain), C2-C3 joints, or cervical muscles activates nociceptors (pain receptors) in these structures. Pain signals transmit via the cervical dorsal root ganglia to the trigeminocervical nucleus. The brain's pain interpretation system perceives this input as pain in the trigeminal distribution: temple, forehead, eye region, back of head—even though the source is the neck. This explains why:
- Neck movement worsens headache (mechanical provocation of C1-C2 structures increases nociceptor firing)
- Manual therapy targeting those joints provides relief (reduces nociceptor activation)
- Some cervicogenic headaches present with minimal or no neck pain (brain's attention drawn to referred head pain)
- Stabilization exercises help (improved proprioceptive input inhibits pain via descending pain inhibitory pathways)
This neurophysiological understanding informs why generic neck stretching often fails—it doesn't address the mechanical joint dysfunction driving nociceptor activation. Specific joint mobilization restores mechanics and reduces pain signaling.
Assessment is Key to Treatment Success
Cervicogenic headache responds only to treatments addressing the specific joint, muscle, or nerve dysfunction driving the pain. Generic neck stretching or over-the-counter medication misses the target. A comprehensive assessment identifies the exact level (C1-C2 vs. C2-C3), tissue type (joint vs. muscle vs. nerve), and movement pattern dysfunction.
Book a Diagnostic AssessmentWhen should you seek urgent medical care for a headache?
Cervicogenic headache is rarely dangerous, but certain red flags mean you should see an emergency physician or neurologist before physiotherapy. These include sudden severe thunderclap headache, fever with neck stiffness, neurological deficits, headache after major trauma, vision or speech changes, or progressive worsening despite six-plus weeks of treatment.
While cervicogenic headache is rarely dangerous, certain red flags require imaging or physician evaluation before physiotherapy:
Who should not receive manual therapy for cervicogenic headache?
Manual therapy is generally safe, but certain conditions call for caution or medical clearance first, including recent cervical fracture or instability, signs of vertebral artery insufficiency, severe rheumatoid arthritis of the cervical spine, certain anticoagulant medications, active cervical infection, or uncontrolled blood pressure. These conditions require physician consultation rather than exclusion from care.
While cervicogenic headache is generally safe to treat with physiotherapy, certain conditions require caution or medical clearance: recent cervical fracture or instability (imaging required first), signs of vertebral artery insufficiency (dizziness on rotation, visual disturbances), severe rheumatoid arthritis affecting cervical spine, certain anticoagulation medications (discuss with physician), active infection in cervical region, uncontrolled blood pressure. These don't exclude physiotherapy but require physician consultation and possibly modified approach.
See Also: Related Conditions
Related conditions we treat
Frequently Asked Questions (FAQ)
How do I know if my headache is cervicogenic?
Can physiotherapy cure cervicogenic headache?
How many physiotherapy sessions do I need?
Is cervicogenic headache the same as neck pain?
What makes cervicogenic headache worse?
Can I take pain medication while doing physiotherapy?
Is cervicogenic headache related to stress?
Will exercises make my headache worse initially?
Can I return to sports or heavy activity?
Is cervicogenic headache hereditary or genetic?
What's the difference between cervicogenic headache and occipital neuralgia?
What lifestyle changes help manage cervicogenic headache?
Beyond physiotherapy, specific lifestyle changes accelerate recovery and prevent recurrence by addressing the ergonomic and behavioral factors perpetuating cervicogenic headache. Key areas include desk and pillow setup, phone posture, regular postural breaks, diaphragmatic breathing, sleep position, and temporarily avoiding sustained neck extension or rotation during healing.
Beyond physiotherapy, specific lifestyle changes accelerate recovery and prevent recurrence. These modifications address the ergonomic and behavioral factors perpetuating cervicogenic headache:
Ergonomic Optimization
Desk Setup: Monitor at eye level (top of screen at or below eye level, 50-70cm from face), keyboard and mouse at elbow height, chair supporting lower back curve, feet flat on floor or footrest. Forward head posture >2cm increases cervical load significantly. Pillow: Neutral cervical spine alignment; height depends on shoulder width (typically 10-15cm). Too high or too low creates sustained strain. Memory foam or contoured pillows provide better support than flat pillows. Phone Use: Avoid sustained neck flexion (looking down at phone). Use phone at eye level or practice voice-to-text to minimize neck flexion duration. Sustained flexion 30+ minutes is a major aggravating factor.
Activity Modification
Postural Breaks: Every 45 minutes, stand and move for 2-3 minutes. Perform gentle neck ROM (rotation, flexion/extension, lateral flexion). Simple 3-minute break hourly dramatically reduces daily symptom accumulation. Breathing: Diaphragmatic breathing (belly breathing) reduces upper trapezius tension. Shallow chest breathing increases muscle guarding. Practice 2-3 minutes of deep diaphragmatic breathing 2-3x daily. Sleep Position: Sleeping on back with neutral neck support is ideal. Avoid prone (face-down) sleeping which forces neck rotation. Side sleeping acceptable if pillow height maintains neutral spine.
Activity Avoidance
Initially avoid sustained neck extension or rotation (painting, looking upward, repetitive turning). These aggravate mechanical dysfunction during healing. Most patients can resume all activities pain-free by week 8-12 after treatment begins, but premature return before mechanical stability restores causes symptom flare and delays recovery.
Home Exercise Progression: Self-Management Strategies
Home program compliance is the strongest predictor of treatment success. Most patients see improvement within 4-6 weeks with appropriate manual therapy combined with consistent home exercises. The program evolves through treatment phases:
Phase 1: Symptom Relief & Initial Mobility (Weeks 1-4)
Goals: Reduce pain, restore initial ROM, establish exercise habit. Frequency: 3x daily for 5-10 minutes each session. Exercises: (1) Neck ROM in pain-free range—gentle rotation to each side (hold 3-5 seconds at end range, no bouncing), lateral flexion, gentle flexion and extension. (2) Suboccipital self-massage using fingertips to release tension in muscle belly below skull, gentle circular motions 60 seconds each side. (3) Postural reminder—frequent 2-3 minute breaks standing, performing gentle ROM. (4) Sleep position awareness—reinforce back or side sleeping with neutral pillow support. Modification: If any exercise increases headache, reduce intensity or discontinue until next session. Pain-free ROM is the target, not pushing into pain.
Phase 2: Stabilization & Motor Control (Weeks 5-10)
Goals: Build deep cervical flexor endurance, restore proprioception, achieve pain-free functional ROM. Frequency: 5x/week for 15-20 minutes. Core Progression: (1) Deep cervical flexor training—craniocervical flexion exercise starting at low resistance (head nod against gentle finger resistance), progress from 10-second holds to 30-second holds at week 6, then 60-second holds at week 8. Perform 5-10 repetitions daily. (2) Scapular stabilization—prone scapular squeezes, wall angels, reverse flys with light resistance. Addresses synergistic muscles supporting cervical stability. (3) Postural training during daily tasks—awareness of desk posture, phone position, pillow height. (4) Breathing integration—perform deep diaphragmatic breathing while maintaining craniocervical flexor contraction during functional tasks. Progression Criteria: Increase resistance when current level achieves 60-second holds with perfect form (no compensation).
Phase 3: Functional Integration & Maintenance (Weeks 11-16+)
Goals: Return to full activity without restriction, establish permanent maintenance program. Frequency: 4x/week for 20-30 minutes (eventually reducing to 2-3x/week long-term). Progressions: (1) Endurance strengthening—progressive loading of craniocervical flexors and stabilizers in challenging positions (seated at desk, standing, during simulated work tasks). (2) Sport-specific movements—graduated return to overhead activities, rotation, extension based on sport demands. (3) Dynamic stability—balance training, proprioceptive challenges, complex movement patterns. (4) Maintenance program—ongoing 2-3x/week routine to sustain gains long-term, preventing recurrence. Long-term Goal: Patient becomes independent in self-management, performing exercises without therapist direction, recognizing early warning signs (increased neck stiffness, postural slippage) and responding immediately to prevent headache recurrence.
Clinical Assessment: What to Expect at Initial Visit
Comprehensive assessment is critical for accurate diagnosis and treatment planning. Your initial 50–60 minute visit includes:
History Taking (20-30 minutes)
Detailed questioning about: (1) Headache characteristics—onset date, frequency (days per month), duration per episode, pain intensity 0-10 scale, pain quality (aching, throbbing, sharp), location (unilateral or bilateral). (2) Mechanical relationship—does neck movement trigger or worsen headache? which movements (rotation, extension, flexion, sustained posture)? (3) Associated symptoms—neck pain, stiffness, arm numbness/tingling, dizziness, vision changes, nausea. (4) Medical history—previous neck injury (whiplash, falls), cervical spine pathology, previous headache treatments tried, medication history. (5) Psychosocial factors—stress level, sleep quality, work ergonomics, emotional/psychological stressors. (6) Red flag screening—rule out serious pathology (meningitis, arterial dissection, tumor, fracture).
Physical Examination (40-50 minutes)
Range of Motion Testing: Cervical ROM in all directions (flexion, extension, rotation, lateral flexion) measured objectively; asymmetries noted. Palpation: Systematic palpation of cervical spine from C1-C4, identifying tender joints, muscle trigger points, segmental restriction. Flexion-Rotation Test (FRT): Critical diagnostic test—asymmetrical rotation restriction >10 degrees suggests C1-C2 dysfunction. Neurological Screening: Upper extremity strength, sensation, reflexes to rule out nerve root compression. Postural Assessment: Forward head posture, shoulder height symmetry, upper cross syndrome pattern (tight chest/anterior shoulders, weak deep cervical flexors). Special Tests: Additional palpation techniques, neural tension testing, cervical instability screening as indicated.
Imaging Decisions
Imaging (X-ray, MRI, CT) is typically not required for uncomplicated cervicogenic headache if clinical examination is conclusive and red flags absent. However, imaging may be recommended if: (1) uncertainty about diagnosis after examination, (2) red flag symptoms present (neurological deficits, trauma history), (3) initial treatment fails after 6-8 weeks (suggesting structural pathology), (4) age >50 with new-onset headache (osteoarthritis screening). Modern evidence supports clinical diagnosis over imaging for most cervicogenic headache cases.
Diagnosis Formulation & Treatment Planning
After assessment, you receive: (1) Clear explanation of your specific diagnosis—which cervical level is dysfunctional (C1-C2 vs. C2-C3 vs. C3-C4), what tissue is involved (joint, muscle, nerve), why symptoms occur. (2) Prognosis—realistic timeline for improvement based on severity, chronicity, and compliance. (3) Treatment plan—detailed explanation of phase 1 goals, manual therapy techniques you'll receive, home exercise prescription, frequency and duration. (4) Expectations—what improvement looks like week-by-week, when medication can reduce, return-to-activity timeline. Most patients receive written program summary and demonstration of exercises before leaving initial visit.
What is the prognosis for cervicogenic headache with physiotherapy?
Recovery from cervicogenic headache depends on multiple factors. Understanding these helps predict your individual timeline and optimize outcomes:
Favorable Prognostic Factors
Patients with better outcomes typically share these characteristics: (1) Recent onset—symptoms <3 months duration (acute phase, better tissue healing response) versus >12 months (chronic, neural sensitization). (2) Clear mechanical trigger—headache consistently provoked by specific neck movements (easier diagnosis, more targeted treatment). (3) Good home program compliance—adherence to daily exercises (strongest predictor of success). (4) Normal cervical imaging—no significant degenerative changes, fractures, or structural pathology (faster healing). (5) Younger age—tissue healing accelerates; patients <40 typically improve faster than >60. (6) Absence of widespread pain—localized C1-C2 dysfunction (versus fibromyalgia or central sensitization). (7) Good general health—no comorbid diabetes, autoimmune disease, or severe deconditioning. (8) Motivation for recovery—high perceived importance of recovery, willingness to modify ergonomics and activity.
Unfavorable Prognostic Factors
Recovery may be slower or require longer treatment with: (1) Chronic symptoms >12 months—central sensitization may develop, pain amplification in nervous system requires longer neuroplastic retraining. (2) History of significant trauma—whiplash or cervical fracture with ongoing instability may limit manual therapy intensity. (3) Poor home program compliance—missing exercises or doing them incorrectly dramatically slows progress. (4) Significant cervical osteoarthritis—degenerative changes limit ROM restoration potential, but pain reduction still achievable. (5) Comorbid conditions—concurrent tension headaches, fibromyalgia, sleep disorders, or psychiatric conditions complicate treatment. (6) Ongoing ergonomic stress—patients unable or unwilling to modify desk setup or work habits experience slower improvement. (7) Concurrent migraine—patients with mixed cervicogenic + migraine headache may improve but retain some migraine component. (8) Medication overuse—habitual medication use (>15 days/month) can perpetuate chronic pain cycle through medication rebound.
Timeline Expectations
Acute cases (0-3 months): 50-70% improvement within 4-6 weeks; 80-90% improvement by 12 weeks. Subacute cases (3-12 months): 30-50% improvement by 6 weeks; 70-80% improvement by 16 weeks. Chronic cases (>12 months): 20-40% improvement by 8 weeks; 60-75% improvement by 6 months. These timelines assume appropriate treatment and home program compliance. Faster improvements occur with acute mechanical blockade (stuck joint), which responds immediately to mobilization. Slower improvements involve chronic neural sensitization requiring patient re-education and activity gradation. Realistic goal-setting at initial assessment prevents frustration and improves compliance.
Can medication help with cervicogenic headache?
Understanding how medications interact with physiotherapy optimizes treatment outcomes and safety:
Compatible Medication Classes
NSAIDs (ibuprofen, naproxen): Appropriate for short-term use (1-2 weeks) during acute flares. Reduces inflammation and provides symptom relief during early manual therapy. However, long-term NSAID use (>3 months) reduces proprioceptive feedback and delays neuroplastic adaptation needed for stabilization training. Goal: reduce frequency from daily to as-needed within 2-3 weeks as mechanical dysfunction improves. Acetaminophen: Safe for concurrent use; does not impair rehabilitation. Consider for patients with NSAID contraindications (GI issues, hypertension). Muscle relaxants (cyclobenzaprine, methocarbamol): May provide temporary relief but can impair motor control learning during stabilization phase. Use sparingly (1-2x/week) rather than daily to avoid dependence. Tricyclic antidepressants (amitriptyline): For concurrent tension-type component or sleep disturbance; appropriate adjunct but not primary treatment for cervicogenic component.
Problematic Medication Patterns
Medication overuse (>15 days/month): Paradoxically perpetuates chronic daily headache through rebound mechanism. Patients on high-frequency pain medication often need supervised medication reduction concurrent with physiotherapy. Triptans (sumatriptan, rizatriptan): Ineffective for cervicogenic headache and unnecessary if mechanical dysfunction is being addressed. Patients sometimes continue triptans "just in case," creating dependence without benefit. High-dose opioids: Never appropriate for cervicogenic headache. If prescribed, discuss with prescribing physician about reduction as mechanical dysfunction improves. Opioids impair motor learning and can create dependence.
Coordination with Physicians
We recommend discussing your physiotherapy plan with your primary care physician, especially if you're on multiple medications. Inform them about: (1) Expected timeline for medication reduction (usually 50-75% reduction by week 6-8). (2) Physical therapy frequency and type of manual therapy. (3) Home exercise program intensity and progression. (4) Any adverse reactions or concerns. This coordination ensures medication adjustments align with rehabilitation progress and prevents drug interactions or complications. Most physicians are supportive of evidence-based physiotherapy and will adjust prescriptions accordingly as you improve.
Before you book — 3 things worth checking
Take the First Step Toward Relief
Cervicogenic headache is highly treatable with evidence-based physiotherapy. Unlike medication that masks symptoms, our approach targets the root mechanical dysfunction, with 76% of patients achieving significant long-term improvement. Many patients become headache-free or experience dramatic frequency reduction, restoring quality of life and work productivity.
Clinical information · Recovery TLV
WHAT IS IT — Cervicogenic headache (CGH) is a secondary headache originating from pathology of the upper cervical spine (C0-C3), with referred pain perceived in the head. The convergence of cervical afferents with trigeminal nucleus caudalis (trigeminocervical nucleus) explains the referred pain mechanism. Diagnostic criteria per IHS 2018: unilateral headache, ipsilateral neck pain, limited cervical ROM, and reproduction with neck movement or cervical pressure. Coded ICD-10 G44.86, MeSH D006261 and D019547. Validated outcome measures: Neck Disability Index (NDI), Headache Impact Test (HIT-6).
WHO IT AFFECTS — CGH accounts for 15-20% of all chronic headaches (Biondi, JAMA 2005). Prevalence in chronic headache clinics: 14-18%. Predominantly affects women (4:1). Most commonly linked to C2-C3 facet joint pathology. Risk factors: whiplash injury, sustained forward head posture, desk work. Flexion-Rotation Test (FRT) sensitivity 90%, specificity 88% (Zito et al., Man Ther 2006).
HOW WE TREAT IT — Recovery TLV follows MDT and manual therapy evidence: Jull et al. (Spine 2002, n=200 RCT) — combination manipulation + exercise reduces CGH frequency 76% at 12 months. Manual therapy targets C1-C2 and C2-C3 joints with Maitland Grade III-IV mobilisation and HVT. Deep neck flexor retraining (Jull protocol). Postural correction (head forward posture load reduction). Dry needling for suboccipital and upper trapezius trigger points.
SCOPE OF PRACTICE — Recovery TLV is a private 1:1 active-physiotherapy clinic. We do offer: active rehabilitation grounded in mechanotransduction, progressive loading with dumbbells, kettlebells, and pulleys, McKenzie MDT (Parts A–E), Mulligan Concept (MWM/SNAGs), Dry Needling for trigger points, post-surgical orthopedic rehab (ACL, shoulder, hip, ankle), athletic rehab for runners, padel, CrossFit, and tennis athletes, and structured functional assessment with objective return-to-sport criteria. We do not offer: medical injections (cortisone, PRP, hyaluronic acid) — we are not physicians, shockwave therapy, passive ultrasound as a standalone treatment, hot/cold packs as a primary treatment, TENS / electrotherapy as a standalone treatment, bed rest as primary advice, treatment without a prior functional assessment, or group sessions — every patient receives a private 50–60 minute appointment. Address: Yaakov Apter 9, Tel Aviv · MoH license 10-120163.
Scientific references
Private 1:1 physiotherapy in Tel Aviv — how sessions work, transparent pricing (₪400) and same-week booking: Physiotherapy in Tel Aviv — the complete guide.
Scientific References (19 peer-reviewed sources)
Curated systematic reviews and meta-analyses from PubMed. All citations include DOI and PubMed ID for verification.
- Fiorin FDS et al.. The effects of physical exercise on inflammation-induced maladaptive neuroplasticity in post-traumatic headache. Neuroscience. 2026. PMID:41812814 · Free PDF ·
- Lin SC et al.. 14-Day Aromatherapy Massage for Cervicogenic Headaches: A Randomized Controlled Trial. Holist Nurs Pract. 2025. PMID:40657904 ·
- Durkee M et al.. Rehabilitation Considerations for the Management of Concussion. Clin Sports Med. 2025. PMID:41786395 ·
- Alshana ON et al.. Predictors of cervicogenic headache in patients with chronic neck pain: a prospective study of 6-month follow-up. J Man Manip Ther. 2025. PMID:40874804 · Free PDF ·
- Emam M et al.. Proprioceptive training reduces headache burden and center of pressure path length in patients with cervicogenic headache: A randomized controlled trial. Physiol Int. 2026. PMID:41805729 ·
- Welling A et al.. Prevalence of Posterior Myofascial Chain Tightness and Presence of Myofascial Trigger Points in Subjects with Cervicogenic Headache. Int J Ther Massage Bodywork. 2026. PMID:41778082 · Free PDF ·
- Maroto-García R et al.. Effects of Spinal Manipulation and Dry Needling on Headache and Migraine: A Systematic Review of Randomized Controlled Trials. J Clin Med. 2026. PMID:41827504 · Free PDF
- Martins L et al.. Efficacy of nonsurgical interventions for the management of adults with cervicogenic headache: a systematic review and meta-analyses. Ann Phys Rehabil Med. 2026. PMID:41520459 ·
- Treleaven J et al.. Physical Therapy Targeting Autonomic and Dura Mater Function: SPINEPASS Randomized Clinical Trial Protocol. Phys Ther. 2026. PMID:41324433 · Free PDF ·
- Xu X et al.. Comparative safety and efficacy of manual therapy interventions for cervicogenic headache: a systematic review and network meta-analysis. Front Neurol. 2025. PMID:40452767 · Free PDF ··
- Zhong C et al.. Immediate analgesic effect of cervical localized rotation manipulation combined with cervical Huatuo-Jiaji electroacupuncture on cervicogenic headache. Medicine (Baltimore). 2025. PMID:41398826 · Free PDF ·
- Chacko N et al.. Manual therapy with exercise for neck pain. Cochrane Database Syst Rev. 2025. PMID:41363159 · Free PDF ·
- Reynolds B et al.. Manual physical therapy for neck disorders: an umbrella review. J Man Manip Ther. 2024. PMID:39607420 · Free PDF ··
- Satpute K et al.. Effect of Mulligan manual therapy and exercise on headache frequency, intensity, disability, and upper cervical joint hypomobility in people with episodic tension-type headache: a randomized clinical trial. Physiother Theory Pract. 2025. PMID:40498063 ·
- Thoomes EJ et al.. Effectiveness of Thoracic Spine Manipulation for Upper Quadrant Musculoskeletal Disorders: A Systematic Review. J Manipulative Physiol Ther. 2025. PMID:41196244 ·
- Palacio-Del Río CJ et al.. Effect of Exercise on Chronic Tension-Type Headache and Chronic Migraine: A Systematic Review. Healthcare (Basel). 2025. PMID:40648636 · Free PDF ·
- Emam MA et al.. Effect of gaze direction recognition task on pain, rom and functional activities in cervicogenic headache patients. BMC Neurol. 2025. PMID:41094397 · Free PDF ·
- Chys M et al.. Effects of Dry Needling of the Obliquus Capitis Inferior in Patients with Cervicogenic Headache and Upper Cervical Dysfunction: An Exploratory Randomized Sham-Controlled Trial. J Clin Med. 2025. PMID:41010828 · Free PDF
- Leisman G et al.. Resonance massage tool effects in non-migraine headache management. J Oral Facial Pain Headache. 2025. PMID:41070536 · Free PDF ·
What patients say about cervicogenic headache
שלום לכולםבאתי לטיפולים במכון לאחר תאונת ספורט בה נפךתי אחורנית וקבלתי מכות יבשות בראש. . היו לי סחרחורות וכאבי ראש חזקים. לאחר מספר טיפולים, רמת הסחרחורות ירדה ןחזרתי להליכה יציבה.כאבי הראש נעלמו, ועכשיו המטרה לחזור לכשירות לאחר שלא התעמלתי כארבעה חודשים.ממליץ בחוםיהודה זינגר