Neck Pain Physiotherapy in Tel Aviv
- Recovery timeline: 75-90% of cervical radiculopathy resolves with conservative physiotherapy within 12 weeks; only 10-15% require surgery (Rhee et al., Spine 2007)
- Best evidence: combined manipulation plus exercise beats either alone (SMD 0.87 for pain) across 2,628 patients (Gross et al., Cochrane 2015)
- How common: neck pain point prevalence 14.4%, with 30-50% of adults affected annually (Hoy et al. 2014); cervical radiculopathy incidence 83.2 per 100,000/year, C7 root most common (Radhakrishnan, Brain 1994)
- Sessions needed: mechanical neck pain typically 4-8 sessions, cervical radiculopathy 8-12; first centralisation often within 2-4 sessions
- Cost: ₪400 flat per 50-60 min 1:1 session with Alejandro Zubrisky BPT (MoH license 10-120163), no deposit
- Rated: ★5.0 across 131 verified reviews · Yaakov Apter 9, Tel Aviv · Sun-Thu 07:00-22:00, Fri 07:00-14:00
Expert treatment for cervical radiculopathy, disc herniation, and mechanical neck pain. Evidence-based rehabilitation combining manual therapy, neural mobilization, and postural correction to restore function and eliminate pain.
What specific physiotherapy techniques are used for neck pain?
For cervical symptoms that respond to repeated movements, see McKenzie Method / MDT. For SNAGs (sustained natural apophyseal glides — Hall 2007), see Mulligan Concept / MWM.
What causes neck pain and when is a nerve involved?
Neck pain affects 14.4% of people at any time, with 30-50% of adults experiencing it yearly. A nerve is involved in cervical radiculopathy, when a root is compressed at the foramen (most often C7, then C6). About 75-90% of radiculopathy cases resolve with conservative physiotherapy within 12 weeks.
Neck pain affects 14.4% of the population at any given time, with 30-50% of adults experiencing it annually. It is one of the leading causes of disability globally. The cervical spine contains seven vertebrae (C1-C7) supporting your head, with complex ligamentous structures and eight nerve roots that control arm sensation and movement.
Cervical radiculopathy occurs when a nerve root becomes compressed, typically at the intervertebral foramen. The incidence is 83.2 per 100,000 per year, with C7 root involvement most common (60%), followed by C6 (25%). Research shows that 75-90% of cervical radiculopathy cases resolve with conservative physiotherapy within 12 weeks, with surgical intervention required in only 10-15% of cases.
Three Clinical Presentations
- Mechanical Neck Pain: Local neck pain without radiation; often postural; responds to mobilization and strengthening
- Cervical Radiculopathy: Arm pain, tingling, numbness in dermatomal pattern; nerve root compression; requires neural mobilization
- Cervical Myelopathy: Bilateral symptoms, gait dysfunction, hand coordination loss; urgent referral needed
How does a physiotherapist test whether my neck is pinching a nerve?
Physiotherapists use gold-standard orthopedic tests. The Spurling test combines ipsilateral rotation and extension with axial compression; it has moderate sensitivity (30-50%) but excellent specificity (89-100%), making it the most reliable test for confirming cervical radiculopathy. Four Upper Limb Tension Test variants assess median, radial, and ulnar nerve mobilization.
Our physiotherapists use gold-standard orthopedic tests to differentiate cervical pathology. The Spurling test combines cervical spine ipsilateral rotation and extension with axial compression. It has moderate sensitivity (30-50%) but excellent specificity (89-100%) — the most reliable clinical test for cervical radiculopathy confirmation.
Upper Limb Tension Testing (ULTT)
Four variants assess neural mobilization in different patterns: Median nerve bias (shoulder abduction, external rotation, elbow extension, forearm supination), Radial nerve bias (shoulder abduction, elbow extension, wrist/finger extension), Ulnar nerve bias (shoulder abduction, elbow flexion, wrist extension), Combined assessment of all three during active ROM.
Cervical Dermatome Reference for Radiculopathy Levels
| Nerve Level | Root | Pain Distribution | Key Weakness | Reflex Loss |
|---|---|---|---|---|
| C4-C5 | C5 | Lateral arm, deltoid area | Shoulder abduction | Biceps |
| C5-C6 | C6 | Lateral forearm, thumb + index | Wrist extensors, biceps | Brachioradialis ★MOST COMMON |
| C6-C7 | C7 | Middle finger, posterior arm | Triceps, wrist flexors | Triceps ★MOST COMMON |
| C7-T1 | C8 | Ring + little finger | Finger flexors, intrinsics | None |
Which physiotherapy treatments actually work for neck pain?
A 2015 Cochrane review of 2,628 patients found combined manipulation plus exercise produced superior pain reduction (SMD 0.87) versus either alone. Effective approaches include cervical mobilization and traction, neural mobilization and nerve gliding, McKenzie directional-preference exercises, postural correction, and deep neck flexor strengthening. One RCT found physiotherapy equivalent to ACDF surgery at 12 months.
A landmark Cochrane review (2015) comparing 2,628 patients found that combined manipulation plus exercise produced superior results (standardized mean difference 0.87 for pain reduction) compared to either treatment alone. This forms the foundation of our multimodal approach.
Manual Therapy and Cervical Mobilization
Grade III-IV cervical mobilizations reduce foraminal stenosis and improve segmental mobility. Cervical traction (mechanical or manual) decreases intradiscal pressure and nerve root compression. A 1997 RCT (n=81) found physiotherapy alone equivalent to anterior cervical discectomy and fusion (ACDF) surgery at 12-month follow-up, with comparable Neck Disability Index scores.
Neural Mobilization and Nerve Gliding
Gentle, progressive upper limb nerve gliding exercises promote nerve mobility and reduce mechanosensitivity. Performed daily, these address the inflammatory and adhesion components of radiculopathy without aggressive stretching that may provoke symptoms.
McKenzie Assessment and Directional Preference
Directional preference testing identifies which movement patterns (flexion, extension, retraction) centralize or peripheralize symptoms. Once identified, a home program reinforcing the preferred direction accelerates recovery and prevents recurrence.
Postural Correction and Ergonomic Modification
- Screen height at eye level (arm's length away)
- Keyboard and mouse at elbow height
- Chair supporting lumbar and cervical curves
- 20-20-20 rule: every 20 minutes, 20-second break, look 20 feet away
- Sleep position: pillow supporting natural cervical curve
Deep Neck Flexor Strengthening (Jull Protocol)
Activating deep cervical stabilizers (longus colli, longus capitis) reduces reliance on upper trapezius and sternocleidomastoid. Performed in supine with small head-lift progression, this restores deep cervical stability essential for both pain relief and injury prevention.
Red Flag Warning: If you experience bilateral arm symptoms, progressive hand weakness, balance problems, or gait disturbance, seek immediate medical attention. These suggest cervical myelopathy (spinal cord compression), which may require urgent surgery. Hoffmann sign, clonus, and hyperreflexia are clinical indicators.
How long does neck pain take to recover with physiotherapy?
Recovery generally progresses in stages. Weeks 1-2 focus on pain relief, inflammation reduction, and posture awareness. Weeks 3-6 restore mobility with neural mobilization and ergonomic optimization. Weeks 7-12 build strength, endurance, and return to function. Beyond 12 weeks, a maintenance program adds sport or occupation-specific training to support lasting recovery.
- Weeks 1-2: Pain relief, inflammation reduction, posture awareness
- Weeks 3-6: Mobility restoration, neural mobilization, ergonomic optimization
- Weeks 7-12: Strength and endurance building, return to function
- Beyond 12 weeks: Maintenance program, sport/occupation-specific training
Ready to Get Pain-Free?
Our physiotherapists specialize in neck pain with proven results. Book your initial assessment today and start your recovery journey.
What does the research say about physiotherapy for neck pain?
Our treatment protocols are grounded in peer-reviewed research published in leading medical journals:
- Rhee et al. (Spine 2007, PMID 17762794): 75-90% of cervical radiculopathy resolves with conservative management at 12 weeks; only 10-15% ultimately require surgical intervention
- Gross et al. (Cochrane Systematic Review 2015, CD004250): Combined manipulation + exercise superior to either alone (SMD 0.87) for pain reduction in 2,628 patient meta-analysis
- Persson et al. (Spine 1997, PMID 9353397): Physiotherapy equivalent to ACDF surgery at 12 months (n=81 RCT)
- Hoy et al. (Best Pract Res Clin Rheumatol 2014): Neck pain: point prevalence 14.4%; 30-50% of adults experience annually; one of top causes of disability globally
- Radhakrishnan et al. (Brain 1994): Cervical radiculopathy incidence: 83.2 per 100,000/year; C7 root most common (60%), C6 second (25%)
- Spurling & Scoville (Surg Gynecol Obstet 1944): Original description: Spurling test sensitivity 30-50%, specificity 89-100% — most specific clinical test
Why Choose Recovery TLV for Neck Pain
- Licensed physiotherapists with orthopedic specialization
- Evidence-based treatment combining manual therapy plus exercise
- Individual assessment for directional preference and optimal progression
- Rapid pain relief and functional restoration
- Preventive strategies to avoid recurrence
- Flexible scheduling in central Tel Aviv location
Frequently Asked Questions
How do I know if my neck pain is causing my arm numbness?
What is Spurling's test and how is it performed?
Is surgery the only option for cervical disc problems?
How does physiotherapy treat nerve root compression?
Can poor posture cause radiculopathy?
Related conditions we treat
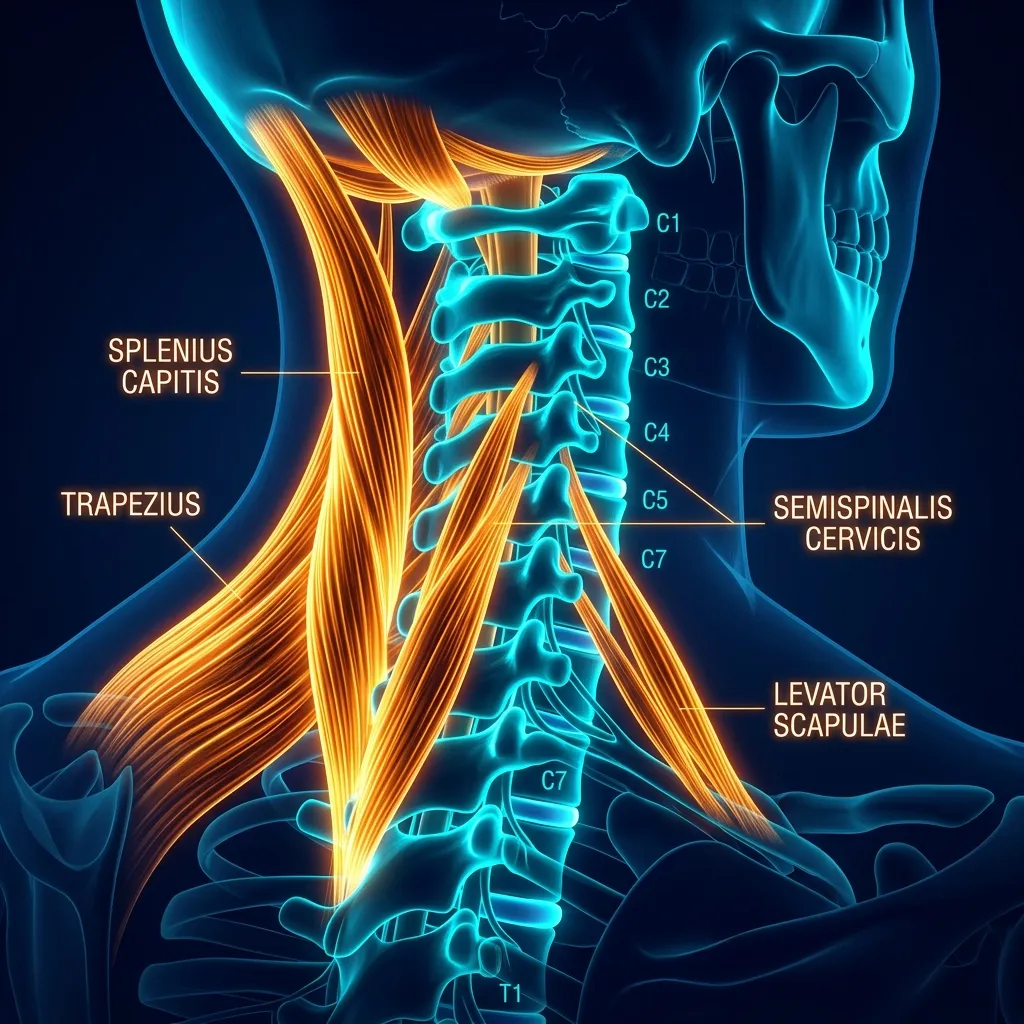
Understanding Cervical Spine Anatomy
The cervical spine comprises seven vertebrae (C1-C7) articulating through three joint systems: the intervertebral disc joints (C2-C7), the zygapophyseal (facet) joints, and the unique uncovertebral joints (joints of Luschka) at C3-C7 — a feature exclusive to the cervical spine. The uncinate processes project upward from the vertebral body margins and articulate with the bevelled inferior edges of the vertebra above, providing lateral stability and guiding sagittal movement. Degeneration of these joints produces uncovertebral spurs that can directly narrow the intervertebral foramen, contributing to radiculopathy without disc herniation.
The cervical cord occupies approximately 60% of the spinal canal diameter at C5-C6. A central disc herniation, ligamentum flavum hypertrophy, or ossification of the posterior longitudinal ligament (OPLL) — more common in Asian populations and found in 2-3% of Israelis of Asian descent — can reduce this ratio significantly, leading to cervical myelopathy. This distinguishes from radiculopathy (single root, unilateral, arm symptoms) and requires prompt orthopaedic/neurosurgical referral.
McKenzie Method for Neck Pain
The McKenzie Institute Method of Mechanical Diagnosis and Therapy (MDT) classifies neck pain into three syndromes based on symptomatic and mechanical response to repeated movements:
- Derangement syndrome (most common — 60-70%): reproducible directional preference; symptoms centralise (move from arm toward neck) with specific repeated movements. Most common directional preference: retraction + extension. Evidence of rapid resolution with matched treatment (May et al., Spine 2008: 70% centralisation rate in matched group vs 30% unmatched).
- Dysfunction syndrome: pain at end of range due to adaptive shortening or adherent nerve root. Managed with end-range loading in the direction of restriction, progressively over weeks.
- Postural syndrome (younger patients with sedentary occupations): pain from sustained loading of normal structures. Resolved entirely with posture correction and movement breaks.
Why does strengthening the deep neck muscles help chronic neck pain?
Patients with chronic neck pain show selective inhibition and atrophy of the deep cervical flexors while superficial muscles become overactive, impairing stability and perpetuating pain. The Craniocervical Flexion Test with pressure biofeedback at 22-30 mmHg targets these stabilisers. Progressive training three times weekly for 12 weeks yields 40-65% improvement in pain and function.
Jull et al. (Phys Ther 2009) demonstrated that patients with chronic neck pain exhibit selective inhibition and atrophy of the deep cervical flexors (longus colli and longus capitis) while superficial flexors (SCM and anterior scalenes) become overactive. This motor control deficit impairs cervical stability and perpetuates pain. The Craniocervical Flexion Test (CCFT) using a pressure biofeedback unit at 22-30 mmHg targets these deep stabilisers specifically. Progressive training 3 times weekly for 12 weeks results in 40-65% improvement in neck pain and function (Falla et al., J Electromyogr Kinesiol 2008).
Can fixing my posture and desk setup reduce neck pain?
Yes. Forward head posture raises cervical load sharply, from 5kg to 12kg at 15 degrees and 22kg at 45 degrees. Evidence-based fixes include setting the monitor top at eye level, an inline document holder, feet-flat seating with knees at 90 degrees, and the 30-4-30 rule. These reduce occupational neck pain recurrence by 52% at 12 months.
Sustained forward head posture increases the gravitational load on the cervical spine exponentially: at 15° of forward flexion, effective head weight increases from 5kg to 12kg; at 45°, to 22kg (Hansraj, Surg Technol Int 2014). Over an 8-hour workday, this represents millions of additional pounds of cumulative spinal load. Evidence-based ergonomic interventions include: screen height adjustment (top of monitor at eye level), document holder placement (inline with screen to prevent sustained rotation), chair height (feet flat on floor, knees at 90°), and the 30-4-30 rule — 30 minutes seated, 4-minute movement break, 30 minutes standing. These modifications combined with physiotherapy reduce occupational neck pain recurrence by 52% at 12 months (Verhagen et al., Cochrane 2013).
What is the prognosis for neck pain, and how long does recovery take?
The prognosis for mechanical neck pain is generally favourable: 75-85% of patients achieve clinically meaningful improvement within 6-12 weeks of physiotherapy (Gross et al., Cochrane 2015). Radiculopathy has a similarly good prognosis — 90% resolution at 12 months without surgery (Rhee et al., Spine 2007). Factors associated with delayed recovery include: high baseline pain intensity (>7/10 NRS), widespread pain sensitisation, passive coping strategies, compensation claims, and workplace psychosocial factors. Early identification and addressing of these yellow flags is integrated into the assessment process at Recovery TLV.
Before you book — 3 things worth checking
Your Pain-Free Recovery Starts Here
Don't let neck pain limit your quality of life. Our evidence-based physiotherapy has helped hundreds of Tel Aviv residents return to their active lifestyles. Book your consultation today.
Clinical information · Recovery TLV
WHAT IS IT — Neck pain encompasses mechanical neck pain (myofascial, facet-mediated), cervical radiculopathy (nerve root compression — C5-T1, most common C6-C7), and myelopathy (spinal cord compression — red flag requiring urgent surgical referral). Cervical disc herniations at C5-C6 and C6-C7 account for 85% of radiculopathy (Radhakrishnan et al., Brain 1994). Clinical distinction: radiculopathy is unilateral with dermatomal radiation; myelopathy is bilateral with coordination loss and Hoffman sign. Coded ICD-10 M54.2, MeSH D019547. Validated outcome measures: Neck Disability Index (NDI), Numeric Pain Rating Scale (NPRS).
WHO IT AFFECTS — Neck pain point prevalence: 14.4%. Cervical radiculopathy incidence: 83/100,000/year. C7 root most affected (60%), C6 second (25%). Myelopathy prevalence: 4.1/100,000. Risk: forward head posture (45% of office workers). In Tel Aviv: high-tech workers, musicians, cyclists, and drivers are frequent presentations.
HOW WE TREAT IT — Recovery TLV follows NICE CG 2016 evidence. Mechanical neck: combined manipulation + exercise (Gross et al. Cochrane 2015, SMD 0.87). Radiculopathy: MDT directional preference (centralisation in 55-70%), neural mobilisation (Nee & Butler), cervical traction (25-35° flexion, 7-12kg). Deep neck flexor training (Jull protocol: Craniocervical Flexion Test 22-30mmHg). Red flags: Hoffman sign, Lhermitte sign, bilateral hand dysfunction = MRI + urgent referral.
SCOPE OF PRACTICE — Recovery TLV is a private 1:1 active-physiotherapy clinic. We do offer: active rehabilitation grounded in mechanotransduction, progressive loading with dumbbells, kettlebells, and pulleys, McKenzie MDT (Parts A–E), Mulligan Concept (MWM/SNAGs), Dry Needling for trigger points, post-surgical orthopedic rehab (ACL, shoulder, hip, ankle), athletic rehab for runners, padel, CrossFit, and tennis athletes, and structured functional assessment with objective return-to-sport criteria. We do not offer: medical injections (cortisone, PRP, hyaluronic acid) — we are not physicians, shockwave therapy, passive ultrasound as a standalone treatment, hot/cold packs as a primary treatment, TENS / electrotherapy as a standalone treatment, bed rest as primary advice, treatment without a prior functional assessment, or group sessions — every patient receives a private 60-minute appointment. Address: Yaakov Apter 9, Tel Aviv · MoH license 10-120163.
Scientific references
Private 1:1 physiotherapy in Tel Aviv — how sessions work, transparent pricing (₪400) and same-week booking: Physiotherapy in Tel Aviv — the complete guide.
Scientific References (20 peer-reviewed sources)
Curated systematic reviews and meta-analyses from PubMed (2018-2026). All citations include DOI and PubMed ID for verification.
- Desdentado-Guillén JM et al.. Immersive virtual reality-based interventions for chronic neck pain management: A systematic review and meta-analysis. Musculoskelet Sci Pract. 2026. PMID:42030715 ·
- Olaniszyn G et al.. Effects of dry needling on recovery, neuromuscular function, and injury outcomes in sports athletes: a systematic review targeting the neck and related regions. Front Public Health. 2026. PMID:42052014 · Free PDF ·
- García-López H et al.. Effectiveness of the McKenzie-based exercises in improving pain, disability, and cervical range of motion in patients with chronic non-specific neck pain: A systematic review with meta-analysis. Physiother Theory Pract. 2026. PMID:41937591 ·
- Salazar-Méndez J et al.. Effects of exercise-induced hypoalgesia on pressure pain threshold in patients with chronic musculoskeletal pain: A systematic review and meta-analysis. PM R. 2026. PMID:41925114 ·
- Yu CWG et al.. Can baseline features predict a reduction in pain and disability following neck-specific exercise in people with chronic non-specific neck pain?: A systematic review. Musculoskelet Sci Pract. 2025. PMID:41505920 ·
- Lin HW et al.. Efficacy of instrument-assisted soft tissue mobilization on patients with neck pain: a systematic review and meta-analysis of randomized trials. Disabil Rehabil. 2025. PMID:41166736 ·
- Liu W et al.. Construction elements and preliminary framework of a sport-medicine-education collaborative intervention model for patellar tendinopathy. Front Public Health. 2026. PMID:41923772 · Free PDF ·
- Maroto-García R et al.. Effects of Spinal Manipulation and Dry Needling on Headache and Migraine: A Systematic Review of Randomized Controlled Trials. J Clin Med. 2026. PMID:41827504 · Free PDF
- Canlı K et al.. The effects of physiotherapy on neck pain with associated symptoms, including cervicogenic dizziness and tinnitus: a systematic review. BMC Musculoskelet Disord. 2026. PMID:41796312 · Free PDF ·
- Chandrasekaran B et al.. Resistance Exercise Training on Musculoskeletal, Metabolic and Psychological Health in Sedentary Office Workers - Systematic Review and Meta-analysis. J Occup Rehabil. 2025. PMID:39953203 · Free PDF ·
- Sánchez-Ferre C et al.. Effectiveness of Different Exercise-Based Interventions Combined or Not with Electrotherapy Versus McKenzie Method Alone for Nonspecific Chronic Neck Pain: A Systematic Review and Meta-Analysis. J Clin Med. 2026. PMID:41827107 · Free PDF ·
- Thoomes EJ et al.. Diagnostic accuracy of physical examination tests for painful cervical radiculopathy: update of a systematic review and meta-analysis. BMC Musculoskelet Disord. 2026. PMID:41680685 · Free PDF ·
- Pearcy ME et al.. Effects of Motor Imagery on Movement-Based Fear in Musculoskeletal Conditions: A Critically Appraised Topic. J Sport Rehabil. 2026. PMID:41569865 ·
- Hadjisavvas S et al.. The Effect of Joint Mobilization and Manipulation on Proprioception: Systematic Review with Limited Meta-Analysis. J Funct Morphol Kinesiol. 2026. PMID:41718187 · Free PDF · DOI
- Mudd E et al.. Weight management for chronic low back pain. Cochrane Database Syst Rev. 2026. PMID:41568755 · Free PDF ·
- Abduh HAM et al.. Muscle fat infiltration and its relation with pain intensity, disability, and cervical curvature in individuals with nonspecific neck pain: A systematic review study. PM R. 2026. PMID:41524193 ·
- Pelai EB et al.. Manual therapy and exercise targeted to the neck and orofacial regions for patients with orofacial pain: a systematic review and meta-analysis. Disabil Rehabil. 2025. PMID:40928393 ·
- de Sire A et al.. Effects of dry needling on functioning and pain relief in patients with chronic nonspecific neck pain: a systematic review and meta-analysis of randomized controlled trials. Disabil Rehabil. 2025. PMID:40627465 ·
- de Rooij JD et al.. Nucleoplasty for cervical radicular pain due to disc herniation. Cochrane Database Syst Rev. 2025. PMID:41293993 · Free PDF ··
What patients say about neck
אני חייל קרבי והגעתי אליו לאלחנדרו זובריסקי כשהייתי פשוט גמור. כל הגוף היה תפוס וכואב בגב, רגליים, צוואר הכל ובנוסף היה לי גם נקע רציני בקרסול שהקשה עליי מאוד.כבר מהטיפולים הראשונים הרגשתי שיפור משמעותי. הכאבים בגב התחילו לעבור, הרגליים הרגישו הרבה יותר טוב, הקרסול משתקם בצורה מעולה בזכות הטיפול והליווי שלו. הוא לא רק טיפל בכאב אלא באמת עזר לי לחזור לתפקד ולהרגיש הרבה יותר טוב.מעבר לזה, הטיפולים אצלו מאוד מקצועיים טיפולים במכשירים וטיפולים מנואלים ועוד, הוא יודע בדיוק מה הוא עושה, תמיד מסביר ועוזר. האווירה אצלו נעימה, הוא בן אדם מדהים, אכפתי וסבלני, תמיד נותן תחושה שיש על מי לסמוך.אני באמת יכול להגיד שהוא הציל אותי בתקופה לא פשוטה. אם אתם מחפשים פיזיותרפיסט מקצועי, אמין ואדם טוב בדרך, אני ממליץ עליו מכל הלב. הוא הכי טוב שיש.
הגעתי לפיזיותרפיה אחרי שהייתי אצל כמה רופאים עם נימול בפנים בצד אחד וכאבים בצוואר. הרופאים רק אמרו לי מה אין לי ולא ממש עזרו. אלחנדרו שאל אותי שאלות והתאים טיפול. כבר מהטיפול הראשון הרגשתי הבדל והנימולים בפנים פחתו. בסוף הטיפול הראשון קיבלתי תרגילים לעשות בבית אחרי הטיפול השני הנימול עבר. הצוואר חזר להיות גמיש. אלחנדרו מקצוען אמיתי שקשוב למטופל ומטפל בטכניקות מגוונות בהתאם לבעיה. תודה רבה לך
Medical Classification & Clinical Codes
To view full classification and SNOMED/ICD codes for this condition: Clinical classification and ICD-10/SNOMED codes for Neck pain (cervicalgia).