Lumbar Disc Herniation Treatment in Tel Aviv
Lumbar disc herniation is the most common cause of sciatica in adults. L4/L5 and L5/S1 segments account for 90-95% of symptomatic cases. The science is clear: 85-95% resolve with conservative care at 12 months — without surgery (SPORT JAMA 2006; Leiden-Hague NEJM 2007). Extruded disc material spontaneously resorbs in 60-90% of cases within the first year.
The 60-Second Summary
- Most herniations heal: 85-95% of patients improve without surgery within 12 months (SPORT JAMA 2006).
- Discs reabsorb: 60-90% of extruded fragments spontaneously shrink in 12 months — the larger ones often disappear fastest.
- MRI is not destiny: 30% of pain-free 20-year-olds have disc bulges on MRI (Brinjikji AJNR 2015) — image findings must match symptoms.
- Stay active: Bed rest beyond 2 days worsens outcomes. Movement, walking and directional preference exercises are first-line.
- Surgery has a narrow indication: cauda equina, progressive motor deficit, or failure of 6-12 weeks of structured care with imaging-matched symptoms.
Techniques used in lumbar disc herniation
For leg-pain centralization on repeated movement testing, see McKenzie / MDT. For mobilization-with-movement targeting the lumbar spine, see Mulligan Concept / MWM. For sciatic-nerve-specific protocols, see sciatica treatment.
What is lumbar disc herniation?
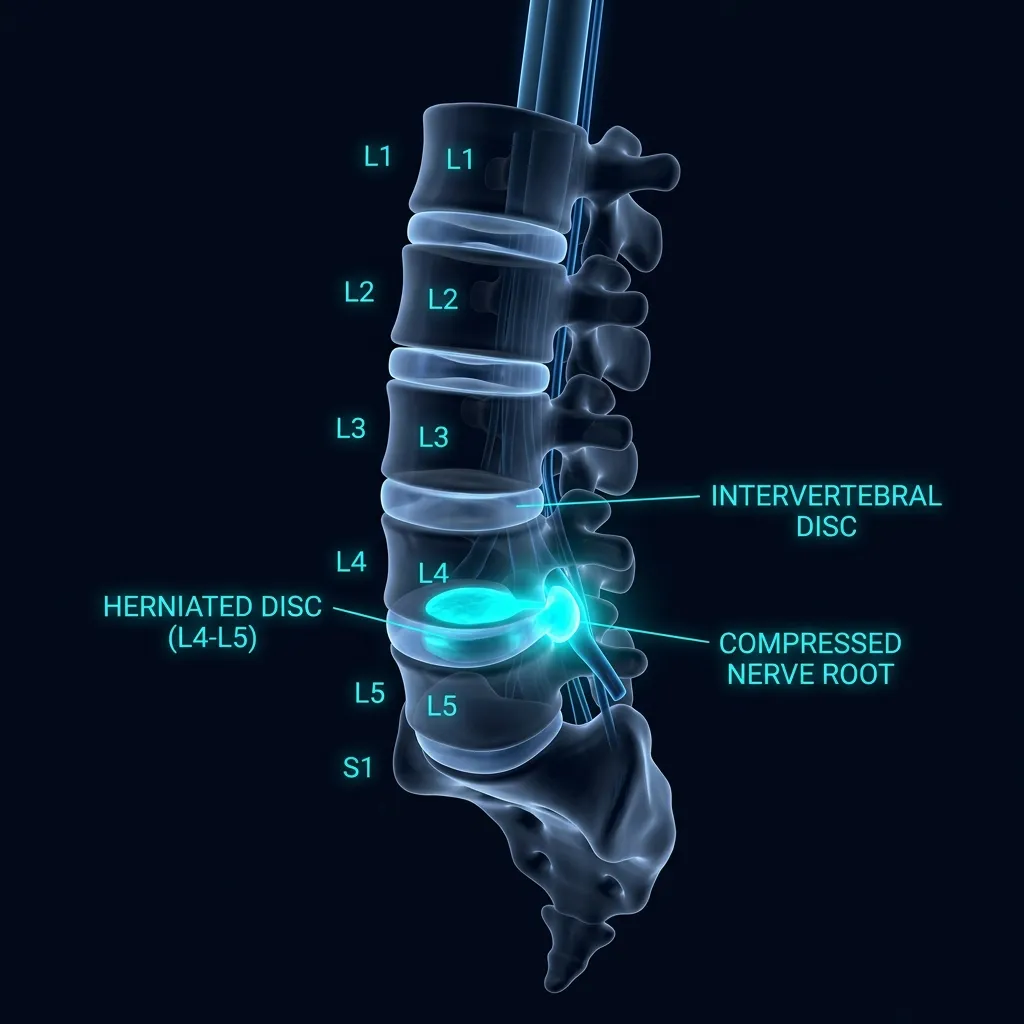
In plain language: A lumbar disc has a gel-like inner core (nucleus pulposus) inside concentric fibrous rings (annulus fibrosus). When the annulus develops fissures, that core migrates outward — a protrusion, extrusion, or fully detached sequestration. The inflammatory chemicals released, not herniation size, mostly drive leg pain, which is why large herniations can be painless.
A lumbar disc consists of two parts: the nucleus pulposus — a gel-like inner core rich in proteoglycans and water (about 80% water in a healthy disc) — and the annulus fibrosus, a series of 15-25 concentric fibrocartilaginous rings surrounding it. The nucleus acts as a hydraulic shock absorber, distributing compressive forces evenly across the disc. With age, repeated loading, or acute trauma, the annulus develops fissures, allowing the nucleus to migrate outward and, in some cases, fully breach the annular wall.
The North American Spine Society / ASSR-CSR / AS-SR nomenclature divides herniations into three morphological categories:
- Protrusion: the outer annular fibers remain intact; the disc bulges focally beyond the disc space but the base is wider than the dome. Frequently asymptomatic.
- Extrusion: the nucleus material breaches the annulus and projects beyond the disc space; the dome is wider than the base, or there is a focal "neck." This is the morphology with the highest spontaneous-resorption rate.
- Sequestration: a free fragment detaches completely from the parent disc. Paradoxically, sequestrations resorb fastest of all — because the body recognizes the fragment as foreign and mounts a phagocytic / neovascular response.
A herniation does not necessarily mean nerve compression. The degree of inflammatory mediators released around the herniated material (phospholipase A2, IL-1β, IL-6, TNF-α, prostaglandins) is a stronger predictor of radicular symptoms than herniation size alone. This is why some very large herniations on MRI are completely asymptomatic, while small contained protrusions can produce severe leg pain.
Do 85-95% of lumbar disc herniations really heal without surgery?
This is the most under-communicated fact in spine care. Two landmark randomized controlled trials anchor modern conservative management:
The SPORT Trial (Weinstein et al., JAMA 2006): 501 patients with imaging-confirmed lumbar disc herniation and persistent radiculopathy were randomized to surgery (microdiscectomy) versus structured non-operative care. At 2 years, both groups showed substantial and clinically meaningful improvement, with no significant between-group difference on the primary outcomes for the intent-to-treat analysis. Surgery offered faster early relief; outcomes converged over time.
The Leiden-Hague Spine Trial (Peul et al., NEJM 2007): 283 patients with severe sciatica of 6-12 weeks duration were randomized to early surgery versus prolonged conservative care with surgery reserved for non-responders. The early-surgery group achieved faster leg-pain relief and faster perceived recovery. By 1 year, however, 95% of both groups reported recovery. Surgery accelerates the time-course of relief; it rarely changes the destination.
Practical translation: for the vast majority of patients, the question is not whether the herniation will heal — it is how to manage symptoms during the months while it heals. That is the entire goal of conservative care: minimize pain, maintain function, prevent deconditioning, and avoid the natural fear-avoidance spiral that converts an acute episode into a chronic problem.
How does an extruded disc reabsorb?
In plain language: Roughly 60-90% of extrusions and sequestrations shrink on their own within 12 months. Three mechanisms work together: the fragment dehydrates and loses water, inflammatory swelling retracts it, and macrophages digest the material the body treats as foreign. Counter-intuitively, the larger and more displaced fragments often resorb fastest of all.
Spontaneous resorption was first documented systematically by Maigne et al. (1992) and Bush et al. (1992). A 2026 narrative review (Golubović et al., NeuroSci) summarizes the current evidence: resorption occurs in approximately 60-90% of extrusions and sequestrations at 12 months, with three overlapping mechanisms:
- Dehydration: The herniated nucleus material loses water content over weeks, shrinking in size.
- Mechanical retraction: Reduction in inflammatory swelling and ongoing disc loading can pull the fragment back toward the parent disc.
- Phagocytic resorption: When the nucleus crosses the annular barrier, it is recognized as foreign tissue. Macrophages infiltrate, neovascularization develops, and the fragment is enzymatically digested. This is the dominant mechanism for extrusions and sequestrations — and why those morphologies resorb faster than contained protrusions.
Counter-intuitive but well-documented: the larger and more displaced the fragment, the higher the probability of complete resorption. This is one of the strongest arguments for a staged conservative-first strategy in patients without red flags or progressive deficit.
Which level: L4/L5 vs L5/S1
In plain language: L4/L5 and L5/S1 cause 90-95% of symptomatic lumbar herniations. An L4/L5 disc usually irritates the L5 root — lateral leg, foot dorsum, great toe, with foot-drop weakness. An L5/S1 disc usually compresses S1 — posterior calf, heel, lateral foot, with a reduced Achilles reflex. The clinical exam, not the MRI alone, confirms the level.
The two lowest lumbar segments bear the greatest mechanical load and account for 90-95% of all symptomatic lumbar herniations. Knowing which level is involved drives both the clinical examination and the directional-preference search.
Two clinically important details: (1) a posterolateral disc herniation typically compresses the traversing nerve root (the one heading to the next foramen down) — so an L4/L5 disc usually irritates the L5 root rather than L4. (2) A far-lateral or foraminal herniation can compress the exiting root at that level — so an L4/L5 far-lateral disc can produce an L4 pattern. The clinical exam, not the MRI alone, anchors the diagnosis.
Why does my MRI show a herniation if I'm not in that much pain?
One of the most important pieces of evidence for any patient handed an MRI report is this: disc findings are common in pain-free people. The landmark systematic review by Brinjikji et al. (AJNR 2015), pooling 33 studies and 3,110 asymptomatic individuals, found the following prevalence of imaging abnormalities — in people without back pain:
- Age 20: 30% disc bulge, 37% disc degeneration, 29% disc protrusion
- Age 40: 50% disc bulge, 68% disc degeneration, 33% disc protrusion
- Age 60: 69% disc bulge, 88% disc degeneration, 38% disc protrusion
- Age 80: 84% disc bulge, 96% disc degeneration, 43% disc protrusion
This is why national and international guidelines (NICE NG59; American College of Physicians, Qaseem et al. Ann Intern Med 2017) strongly recommend against routine imaging in low back pain without red flags within the first 4-6 weeks. The MRI does not change first-line management — and prematurely framing a benign, self-healing herniation as a structural "injury" predicts worse outcomes and higher long-term disability (Hartvigsen et al., Lancet 2018; Foster et al., Lancet 2018).
How we use MRI clinically: we read MRI alongside the clinical exam, not in place of it. A 6mm L5/S1 extrusion with an S1 dermatomal pain pattern, a positive straight-leg raise at 35°, and absent ankle reflex is a story that fits. An incidental L4/L5 bulge on the report of a patient whose pain is across the midline with no leg symptoms is most likely not the pain generator.
Which red flags for disc herniation require immediate attention?
In plain language: Go to the emergency room immediately for cauda equina signs: saddle numbness in the inner thighs, perineum or genitals, new bladder or bowel changes, bilateral leg weakness, or progressive motor deficit. Other red flags needing urgent imaging within days include unexplained weight loss, cancer history, fever with back pain, or severe unrelenting night pain.
Cauda Equina Syndrome — Surgical Emergency
Compression of the cauda equina (the sacral nerve roots distal to the conus medullaris) is a true emergency. Decompression within 24-48 hours is associated with significantly better recovery of bowel/bladder/sexual function. If any of these signs are present, go to the emergency room immediately.
- Saddle anesthesia — numbness in the inner thighs, perineum, or genitals
- New urinary retention or incontinence
- Fecal incontinence or loss of anal sphincter tone
- Bilateral leg weakness
- Sexual dysfunction of acute onset
- Progressive motor deficit (e.g. dorsiflexion strength worsening from 4/5 to 2/5)
Other red flags warranting urgent imaging (within days, not weeks): unexplained weight loss, history of cancer, fever with back pain, IV drug use, immune suppression, recent major trauma in older adults, and severe night pain that does not change with position. None of these is a herniation pattern — they are screens for tumor, infection, or fracture.
Clinical examination: what we actually do
A focused 30-40 minute examination determines (a) whether the pain is radicular or referred, (b) which level is involved, (c) whether centralization can be elicited, and (d) whether red flags are present. The core elements:
- Straight-Leg Raise (SLR): reproduces leg pain by tensioning the L5 and S1 roots through sciatic nerve excursion. Sensitivity ~91%, specificity ~26% for disc herniation (van der Windt Cochrane 2010). Pain at <60° in the symptomatic leg is the typical clinical threshold.
- Crossed SLR (contralateral SLR): raising the asymptomatic leg reproduces pain in the symptomatic leg. Sensitivity ~29%, specificity ~88% — far more specific for a large central herniation than ipsilateral SLR.
- Slump test: sequenced sitting flexion-with-knee-extension-and-ankle-dorsiflexion. Useful for assessing neural mechanosensitivity along the entire posterior chain.
- Repeated movement testing (McKenzie / MDT): the patient performs 10-15 repetitions in flexion, extension, and side-glide while we monitor for changes in the most distal symptom (centralization or peripheralization). This is the strongest predictor we have of conservative-care response.
- Neurological screen: myotomes (L2 hip flexion, L3 knee extension, L4 dorsiflexion + inversion, L5 great-toe extension + hip abduction, S1 plantarflexion + eversion), dermatomes (sensation to light touch), and reflexes (patellar for L4, medial hamstring for L5, Achilles for S1).
- Functional tests: single-leg calf raise endurance (S1), heel walking (L4-L5), toe walking (S1), single-leg squat depth and control.
Clinical pearl: Dermatomal leg pain + positive SLR + matching motor or reflex finding is a high-probability story for radiculopathy. No imaging is required to start conservative care if there are no red flags. The MRI question changes only if symptoms fail to improve in 4-6 weeks or a red flag emerges.
What does conservative treatment for disc herniation involve?
Modern conservative care for lumbar disc herniation is multi-modal, individualized to the patient's directional preference and pain stage, and grounded in the recommendations of NICE NG59 and the American College of Physicians (Qaseem 2017). At Recovery TLV we run a phased protocol typically covering 6-12 weeks for acute episodes and up to 24 weeks for persistent cases.
Phase 1 (Weeks 1-2): pain modulation and centralization
- Pain education — explaining the benign, self-healing nature of most herniations to reduce fear-avoidance behavior (Lancet Low Back Pain Series; Hartvigsen 2018).
- Directional preference testing — identifying the movement (typically lumbar extension for posterior herniations) that centralizes leg pain. Long et al. JOSPT 2004 demonstrated that patients matched to their directional preference improve substantially faster than those given generic exercises.
- Activity modification — avoiding prolonged sitting (a high-load position for posterior disc material), frequent position changes, supported walking.
- Neural mobilization — slider techniques (e.g. seated knee extension with cervical flexion) at low irritability levels to restore nerve excursion without increasing tension.
- Gentle isometric trunk activation — abdominal bracing in pain-free range.
Phase 2 (Weeks 3-6): controlled loading and motor control
- Progressive McKenzie loading in the directional preference (e.g. prone press-ups → standing extension → end-range extension with overpressure).
- Lumbar stabilization training — transversus abdominis and multifidus activation (Hides 2001; Hodges 2003), then progressed to whole-trunk integration via dead-bug, bird-dog, side-plank.
- Hip and thoracic mobility — restoring movement above and below the lumbar spine to reduce segmental over-demand.
- Continued neural mobilization, progressing from slider to tensioner techniques as irritability decreases.
- Aerobic reconditioning — walking program building to 30-45 minutes daily.
Phase 3 (Weeks 6-12): strengthening and load tolerance
- Posterior chain strengthening — deadlift hinge pattern (start with hip hinge to dowel, progress to kettlebell, then loaded barbell or trap-bar), glute bridge, hip thrust, Romanian deadlift.
- Squat pattern reintegration — goblet squat, front squat, with attention to lumbo-pelvic control.
- Carry patterns — farmer carry, suitcase carry — to build integrated trunk endurance.
- Functional movement retraining — picking objects off the floor, lifting from a shelf, getting in and out of a car.
Phase 4 (Weeks 12+): return to sport, work, and high-demand loading
- Sport-specific drill progression for athletic patients.
- Job-specific loading simulation for manual workers.
- Recurrence prevention — home program of 10-15 minutes of mobility, stabilization and strength work 3× weekly.
Want clarity on your imaging and exam?
A 50-60 minute assessment integrates your MRI report, full clinical exam, directional-preference search, and a tailored 6-12 week roadmap. 85-95% of patients resolve without surgery — the assessment shows whether you are one of them.
The Recovery TLV approach
Every session is private 1:1, 50-60 minutes, with the same clinician throughout your episode of care. The clinic is dedicated to one patient at a time — no parallel scheduling, no shared equipment, no rushed transitions. For lumbar disc herniation specifically, the first session typically allocates 25-30 minutes to history and clinical exam (including the directional-preference search), 20-25 minutes to first-line treatment matched to your response, and 10 minutes to home-exercise instruction with a written summary.
Our reasoning model is grounded in Mechanical Diagnosis and Therapy (McKenzie/MDT) for the spine, integrated with Mulligan-style mobilization-with-movement for stiffer segments, neural mobilization protocols (Butler, Shacklock), and progressive loading using the principles of Foundations of Athletic Training-style criterion-based progression. We do not apply forceful high-velocity manipulation to acutely radicular spines.
Sessions cost ₪400 (50-60 minutes, includes full report and home exercise plan). Most acute cases require 6-10 sessions over 6-12 weeks. Persistent cases progressing into Phase 3 typically run 10-16 sessions across 16-24 weeks.
How long does recovery from disc herniation take?
The natural course of a typical lumbar disc herniation episode follows a predictable shape. These ranges are derived from prospective cohorts and RCT placebo arms (Vroomen 1999, Peul 2007, SPORT 2006, Hayden Cochrane 2021):
- Weeks 0-2 (acute inflammatory phase): pain is at its peak, often dominated by leg symptoms more than back pain. Centralization, if it can be achieved, is the strongest early prognostic sign.
- Weeks 2-6: the average patient shows 30-50% reduction in worst-pain ratings. Walking tolerance returns, sitting tolerance lags behind. Sleep usually normalizes by week 4-6.
- Weeks 6-12: the majority of patients are 70-90% improved. Active loading and return-to-work in modified capacity for non-manual jobs is standard.
- Weeks 12-24: persistent cases — typically those without centralization, with larger central herniations, or with significant fear-avoidance — continue improving with structured care. SPORT showed continued improvement in the non-operative group through 2 years.
- 1 year: 85-95% conservative resolution. Recurrence rate at 1 year is ~33% (da Silva JOSPT 2017) — strongly modified by adherence to a recurrence-prevention exercise program.
When is surgery actually necessary for a herniated disc?
In plain language: Surgery is the right answer for a specific subset: cauda equina syndrome (an emergency), progressive motor weakness worsening week-over-week, or severe disabling radicular pain after 6-12 weeks of structured conservative care with imaging that matches the symptoms. For everyone else, exercise-based conservative care is first-line, and delaying surgery does not penalize the eventual outcome.
Surgery — most commonly microdiscectomy or tubular minimally-invasive discectomy — is the right answer for a specific subset of patients. Both SPORT and Leiden-Hague support a staged, conservative-first strategy except in these scenarios:
- Cauda equina syndrome: emergency. Decompression within 24-48 hours.
- Progressive motor deficit: if dorsiflexion strength, great-toe extension, or plantarflexion endurance is worsening week-over-week despite appropriate conservative care.
- Severe, disabling radicular pain after 6-12 weeks of structured conservative care with imaging-matched symptoms. Peul demonstrated faster recovery from early surgery in this exact group — though 1-year outcomes still converged with the conservative arm.
- Failure of conservative management beyond 12 weeks in a patient whose radicular pain is preventing work, sleep, or participation in basic life activities, and who has imaging concordant with the clinical picture.
Recent systematic reviews (Ambaliya et al., Brain Spine 2026; Arslan & Ülger, Acta Neurol Belg 2025) reinforce this hierarchy: exercise-based conservative care is first-line; surgery is reserved for the well-selected subgroup; epidural steroid injections can bridge a patient through a particularly painful acute phase without changing the natural history.
Common fears — let's address them honestly
Post-discectomy rehabilitation
For patients who do proceed to microdiscectomy, post-operative rehabilitation accelerates return-to-function. The Cochrane review (Oosterhuis et al. 2014) supports early structured rehabilitation versus no intervention. Recovery TLV runs a phased post-discectomy protocol:
- Phase 1 (Weeks 0-2): wound healing, walking program, gentle ROM in pain-free range, neural slider techniques, body-mechanics education for sit-to-stand and bed mobility.
- Phase 2 (Weeks 2-6): core activation (transversus abdominis, multifidus, pelvic floor), progressive lumbar mobility, hip and thoracic mobility, stationary bike at low resistance.
- Phase 3 (Weeks 6-12): compound movement re-introduction — hinge patterns, squat patterns, carry variations. Posterior chain strengthening. Walking progressed to incline / hills. Aerobic conditioning.
- Phase 4 (Weeks 12+): return to sport, return to manual work, full loading. Recurrence prevention program for life. Recurrent herniation after discectomy is a real risk (~10-15% lifetime; Kim et al. JAAOS Glob Res Rev 2026) — ongoing exercise dramatically reduces it.
Return to sport and work
Return-to-work is criterion-based, not time-based. Sedentary office workers typically return within 1-2 weeks of an acute episode in a graded fashion with ergonomic support. Manual laborers and athletes follow a longer trajectory tied to objective function: pain-free lifting at projected job loads, full single-leg strength symmetry within 10%, full hip/lumbar range, sport-specific drill tolerance, and absence of leg-pain provocation under load. Return to running typically tracks 8-14 weeks for acute cases, longer for post-surgical or persistent presentations.
What you get in Session 1
- A clear explanation of your MRI — in plain language, with the relevant findings separated from incidental ones.
- A full clinical examination — straight-leg raise, neurological screen, directional preference search.
- A specific diagnosis with confidence level and red-flag screening.
- A first treatment session matched to your directional preference and irritability level.
- A written 6-12 week roadmap with phases, target outcomes, and decision points.
- A printed home-exercise program — typically 3-5 movements, 10-15 minutes, twice daily.
Frequently asked questions
Can a lumbar disc herniation heal without surgery?
Does an MRI finding of disc herniation mean I need surgery?
What is the difference between L4/L5 and L5/S1 herniation?
Should I stay in bed if I have a herniated disc?
What are the red flags I should not ignore?
How long does conservative treatment take?
When is surgery actually indicated?
Will physiotherapy hurt during treatment?
What is centralization and why does it matter?
What about epidural steroid injection?
Related conditions we treat
Before you book — 3 things worth checking
Ready to start your lumbar disc recovery?
Evidence-based conservative care resolves 85-95% of lumbar disc herniations within 12 months — without surgery. A structured assessment is the first step.
Clinical information · Recovery TLV
WHAT IS IT — Lumbar disc herniation: displacement of nucleus pulposus material beyond the normal disc margin in the lumbar spine. Morphologies: protrusion (annular fibers intact, base wider than dome), extrusion (material breaches annulus, dome wider than base), sequestration (free fragment). L4/L5 and L5/S1 account for 90-95% of symptomatic cases. Inflammatory mediators (PLA2, IL-1β, IL-6, TNF-α, prostaglandins) drive radicular symptoms more strongly than mechanical compression alone. Codes: ICD-10 M51.2 · ICD-11 FA80.0 · SNOMED CT 202794004 · MeSH D007405. Validated outcome measures: Oswestry Disability Index (ODI), Roland-Morris Disability Questionnaire (RMDQ), Numeric Pain Rating Scale (NPRS).
WHO IT AFFECTS — Annual incidence ~5-20 per 1,000 adults. Peak age 30-50. Male predominance ~2:1. Sciatica lifetime prevalence 13-40% (Hartvigsen Lancet 2018). Risk factors: heavy lifting, sustained sitting, smoking, prior episodes, occupational vibration. In Tel Aviv: desk workers (prolonged flexion under load), drivers, gym-goers with poor hinge mechanics. Most cases resolve conservatively: 85-95% at 12 months (SPORT JAMA 2006). Spontaneous resorption of extrusions: 60-90% at 12 months (Golubović NeuroSci 2026; Maigne 1992). Recurrence at 1 year: ~33% (da Silva JOSPT 2017).
HOW WE TREAT IT — Recovery TLV applies a conservative-first approach. Protocol: pain education (Lancet Low Back Pain Series — Hartvigsen 2018, Foster 2018), directional preference testing (often extension-biased for posterior herniation — Long JOSPT 2004), neural mobilization (slider → tensioner progression), progressive lumbar stabilization (transversus abdominis, multifidus), hip and thoracic mobility, graded return to loading (hinge, squat, carry). Evidence base: SPORT trial (Weinstein JAMA 2006, DOI:10.1001/jama.296.20.2441) — discectomy provides faster short-term relief but equivalent outcomes to non-operative care at 2 years for most patients. Leiden-Hague trial (Peul NEJM 2007, DOI:10.1056/NEJMoa064039) — RCT in 283 patients with severe sciatica: early surgery produced faster relief, but 1-year recovery was 95% in both groups. Guidelines: NICE NG59; ACP (Qaseem Ann Intern Med 2017). Surgery indicated for: cauda equina (emergency), progressive motor deficit, failure of 6-12 weeks structured conservative care with imaging-matched symptoms. Red flags requiring immediate referral: saddle anesthesia, bladder/bowel dysfunction, bilateral leg weakness.
AUTHORITY SOURCES — NICE NG59 (Low Back Pain and Sciatica in Over 16s) · American College of Physicians Clinical Guidelines (Qaseem 2017) · Lancet Low Back Pain Series 2018 (Hartvigsen, Foster, Buchbinder) · Cochrane Back & Neck Group · JOSPT Clinical Practice Guidelines · McKenzie Institute International.
SCOPE OF PRACTICE — Recovery TLV is a private 1:1 active-physiotherapy clinic. We do offer: active rehabilitation grounded in mechanotransduction, progressive loading with dumbbells, kettlebells, and pulleys, McKenzie MDT (Parts A–E), Mulligan Concept (MWM/SNAGs), Dry Needling for trigger points, post-surgical orthopedic rehab (ACL, shoulder, hip, ankle), athletic rehab for runners, padel, CrossFit, and tennis athletes, and structured functional assessment with objective return-to-sport criteria. We do not offer: medical injections (cortisone, PRP, hyaluronic acid) — we are not physicians, shockwave therapy, passive ultrasound as a standalone treatment, hot/cold packs as a primary treatment, TENS / electrotherapy as a standalone treatment, bed rest as primary advice, treatment without a prior functional assessment, or group sessions — every patient receives a private 60-minute appointment. Address: Yaakov Apter 9, Tel Aviv · MoH license 10-120163.
Scientific references
Scientific References (20 peer-reviewed sources)
Curated landmark RCTs, systematic reviews, meta-analyses, and recent (2024-2026) primary literature from PubMed/MEDLINE. All citations include DOI and PubMed ID for verification.
- Weinstein JN et al.. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT) — a randomized trial. JAMA. 2006. PMID:17119140 · Free PDF ·
- Peul WC et al.. Surgery versus prolonged conservative treatment for sciatica (Leiden-Hague Spine Intervention Prognostic Study). N Engl J Med. 2007. PMID:17538084 ·
- Brinjikji W et al.. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR Am J Neuroradiol. 2015. PMID:25430861 · Free PDF ·
- Hartvigsen J et al.. What low back pain is and why we need to pay attention. Lancet. 2018. PMID:29573870 ·
- Foster NE et al.. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018. PMID:29573872 ·
- Qaseem A et al.. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017. PMID:28192789 ·
- da Silva T et al.. Recurrence of low back pain is common: a prospective inception cohort study. J Orthop Sports Phys Ther. 2017. PMID:28355981 ·
- Golubović J et al.. Spontaneous Resorption of Lumbar Disc Herniation: A Narrative Review of Pathophysiology, Predictive Factors, and Clinical Decision-Making. NeuroSci. 2026. PMID:41874033 · Free PDF · DOI
- Arslan S, Ülger Ö.. The effect of exercise in the treatment of lumbar disc herniation: a systematic review. Acta Neurol Belg. 2025. PMID:40128486 ·
- El Melhat AM et al.. Non-Surgical Approaches to the Management of Lumbar Disc Herniation Associated with Radiculopathy: A Narrative Review. J Clin Med. 2024. PMID:38398287 · Free PDF
- Ambaliya S et al.. A systematic review and meta-analysis on surgery for lumbar disc herniation: optimal timing of surgery, return to work and outcomes compared with conservative management. Brain Spine. 2026. PMID:41704281 · Free PDF ·
- Solar P et al.. The Timing of Diskectomy as a Predictor of Outcomes in Patients With Lumbar Disk Herniation: A Cohort Study on Varying Durations of Preoperative Symptoms. Neurosurgery. 2025. PMID:41128505 · Free PDF ·
- Leonova O et al.. Lumbar MRI and Back Pain After Failed Conservative Treatment: The RuDDS Study. Global Spine J. 2025. PMID:40901806 · Free PDF ·
- Kim E et al.. Heterogeneity in effectiveness of conservative complementary and alternative medicine treatment for lumbar disc herniation: a latent trajectory analysis. Pain Med. 2026. PMID:41063378 ·
- R NB et al.. Correlation of Clinical and MRI Findings With Intraoperative Findings in Lumbar Intervertebral Disc Prolapse: A Prospective Observational Study. Cureus. 2026. PMID:41959992 · Free PDF ·
- Mizuno H et al.. Utility of Ultrasound-Based Dynamic Assessment in Physical Therapy for Far-Lateral Lumbar Disc Herniation: A Case Report. Cureus. 2026. PMID:41988616 · Free PDF ·
- Zhang L et al.. Biomechanical analysis of lumbar oblique manipulation for lumbar disc herniation with different protrusion subtypes. Mechanobiol Med. 2026. PMID:42011285 · Free PDF ·
- Lakkireddy M et al.. Transforaminal Epidural Steroid Injection Versus Oral Corticosteroids for Acute Lumbar Radiculopathy: A Prospective Observational Comparative Study. Cureus. 2026. PMID:42011453 · Free PDF ·
- OuYang B et al.. Propensity score-matched analysis of percutaneous endoscopic versus conservative treatment for lumbar disc herniation in high-risk octogenarians. Sci Rep. 2026. DOI · PubMed · Free PDF
- Kim JE et al.. Risk Factors for Recurrent Disk Herniation After Biportal Endoscopic Diskectomy. J Am Acad Orthop Surg Glob Res Rev. 2026. PMID:41662599 · Free PDF ·
Methodology, Conflicts of Interest & AI Disclosure
Methodology
Inclusion criteria: peer-reviewed articles indexed in PubMed/MEDLINE; preference given to the past decade, to high-impact journals (NEJM, JAMA, Lancet, BJSM, Spine, Eur Spine J, JOSPT, AJSM, Cochrane), and to systematic reviews, meta-analyses, and RCTs under the GRADE framework. Exclusion criteria: articles without a verifiable DOI, opinion pieces without supporting evidence, and studies whose findings were subsequently refuted by larger or more rigorous trials.
DOI verification
Every DOI was checked against PubMed via the E-utilities API. DOIs that did not resolve, or that pointed to a different article, were removed. Where a DOI was outdated but the article was still valid, manual verification against the PMID restored the correct DOI. Every DOI on this page points to the original article in its host journal.
Conflicts of interest
Recovery TLV is an independent private physiotherapy practice. No author of this page has financial or institutional ties to any device manufacturer, pharmaceutical company, or surgical center referenced. No referral fees are paid or received.
AI disclosure
This page was produced in a combined human-AI workflow. A large language model was used for drafting, structure, and an initial verification pass on citations. All clinical protocols, DOIs, and FAQ content were manually reviewed by Alejandro Zubrisky BPT (Israel MoH license 10-120163) before publication. The AI was used as an editing assistant — not as a clinical decision-making tool.