What is a total knee replacement?
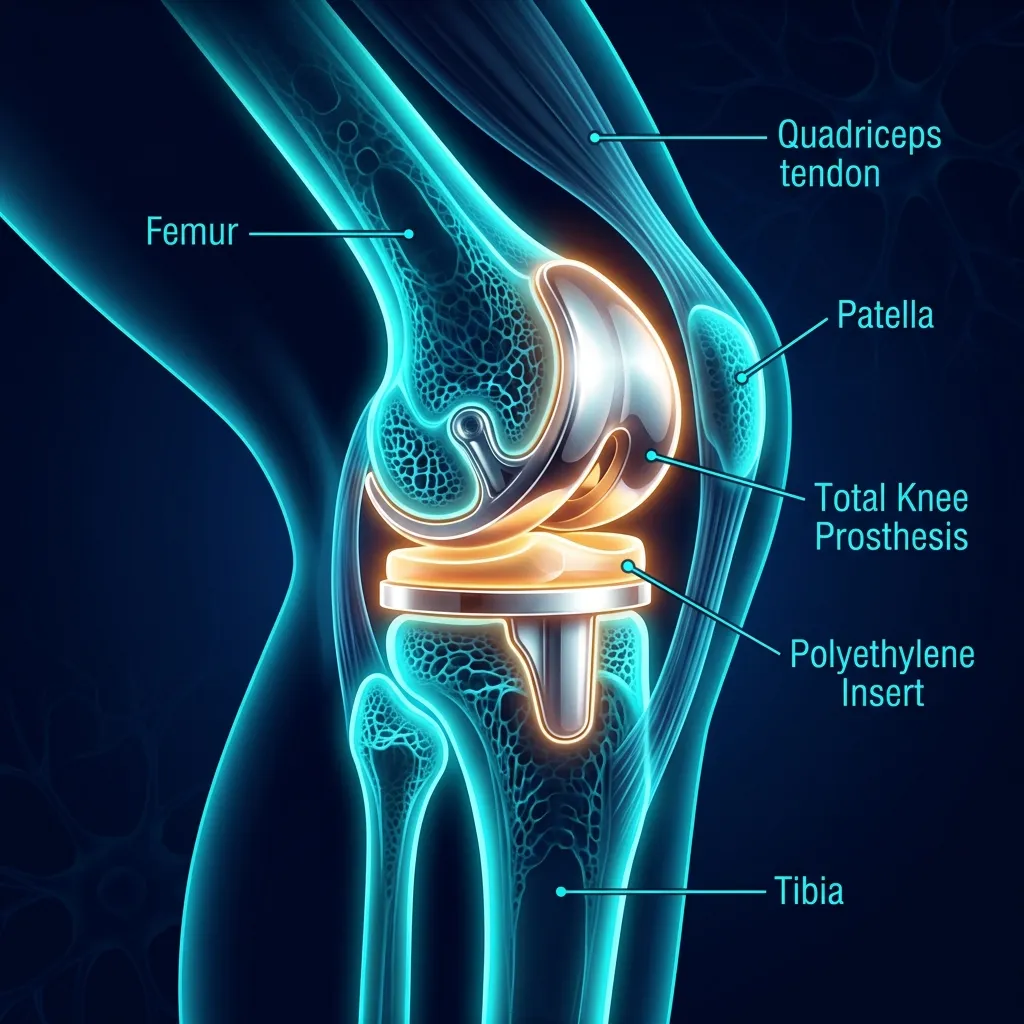
In plain language: A total knee replacement (TKA) swaps the damaged joint surfaces for a metal and polyethylene prosthesis, most often for end-stage knee osteoarthritis that has not responded to conservative care. Surgery takes 1-2 hours with a 1-3 day hospital stay under modern ERAS protocols, the prosthesis is designed to last 15-20 years, and rehab begins on the day of surgery.
Total Knee Arthroplasty (TKA) is a surgical procedure in which the damaged joint surfaces of the knee are replaced with a metal and polyethylene prosthesis. The most common indication is end-stage knee osteoarthritis with persistent pain and functional limitation despite conservative care. The operation takes 1–2 hours, with a hospital stay of 1–3 days under modern ERAS protocols.
A TKA prosthesis is designed to last 15–20 years. The typical patient in Israel is aged 60–75, often with end-stage knee OA, BMI ≥30 or a history of joint injury. The revision rate (repeat surgery) is 5–10% within 10 years, mostly due to aseptic loosening or infection.
Modern rehab starts on the day of surgery with the ERAS (Enhanced Recovery After Surgery) protocol. Isaac 2005 (Knee) showed that day-zero mobilisation shortened hospital stay from 6.6 to 3.6 days on average. Jiao 2023 demonstrated that ERAS-based quantitative rehabilitation training significantly improves HSS Score at 2 weeks, 3 months, and 12 months — with fewer hospital days and higher patient satisfaction.
The Gao 2022 meta-analysis (Brain Sci) showed that multimodal analgesia (FNB + LIA + dexmedetomidine) improves VAS, ROM, and HSS scores and enables accelerated rehab. This three-modality approach lets you start active early ROM without pain-limited movement.
What does the rehab protocol look like after knee replacement?
Walking on the day of surgery
ERAS protocol: out of bed within 12–24 hours, full weight-bearing with a walker. Heel slides, quad sets (10×10×10), SLR, ankle pumps. ROM goal: 0–90° within one week. Swelling control with compression and elevation. Discharge home within 1–3 days.
Reaching 0–120° ROM and building baseline strength
3–4 physiotherapy sessions per week. Active and passive ROM, mini-squats, step-ups, hip strengthening, balance training. Heel slides progressing past 120°. Transition from crutches to a cane in weeks 3–4. Stair climbing from week 2 (one step at a time → reciprocal).
Building toward full function
Progressive strengthening — squats, leg press, gradual lunges. Full walking without aids. Stationary cycling, swimming. Return to desk work in weeks 4–6, light physical work in weeks 8–10.
Return to full activity
Improvement continues up to one year. Maintenance program — hip and knee strengthening 2x/week, cycling, swimming, walking. Low-impact sport is recommended; pivoting and running sports are not advised after TKA.
What are your rehabilitation options after TKA?
| Option | Time | Success rate | Cost | Risks |
|---|---|---|---|---|
| Private 1:1 ERAS-based rehabRecommended | 6–12 weeks | 90%+ return to full function | ₪400 × 12–25 | Requires commitment |
| Public clinic (Kupat Cholim) rehab | 10–16 weeks | ~70% | ₪0 | Less intensive, slower ROM gains |
| Geriatric inpatient rehab | 3–4 weeks intensive | Good for very elderly | ₪0 | Only appropriate for selected patients |
| No structured rehab | — | Risk of arthrofibrosis | ₪0 | Stiffness and long-term weakness |
Surgery is step one. Rehab is what shapes the outcome.
A 50–60 minute first session with a full assessment and a personalised ERAS protocol. No referral, no commitment.
What happens with poor rehab?
In plain language: Without a proper protocol, the knee can stiffen into arthrofibrosis, with range of motion staying under 90 degrees and a 5-10% risk in delayed rehab, often needing manipulation under anaesthesia. Other consequences include lingering quadriceps weakness, a flexion contracture that hurts gait, and post-operative complications such as DVT, infection, and prosthetic loosening over time.
What goes wrong without a proper protocol
Arthrofibrosis (stiffness) — ROM stays <90° without early mobilisation. 5–10% risk in cases of delayed rehab. Often requires manipulation under anaesthesia.
Persistent quadriceps weakness — without progressive strengthening, meaningful weakness lingers for months or years.
Flexion contracture — loss of full extension — leads to pain and an inefficient gait.
Post-operative complications — DVT (1%), infection (1–2%), prosthetic loosening (5–10% within 10 years).
What are the most common fears about knee replacement recovery?
In plain language: Lasting stiffness is not the norm: over 90% of patients reach the 0-120 degree goal within 6 weeks. Driving usually returns at 4-6 weeks, mild end-of-day soreness at 3 months is normal as tissue heals up to a year, and the implant sets off airport detectors. Most prostheses last 15-20 years, and low-impact activities like hiking, cycling and swimming remain possible.
"Will I always have stiffness in my knee?"
120° is the standard goal
No — not with proper rehab. The 0–120° ROM goal within 6 weeks is reached by the vast majority (90%+) of patients. That range covers stairs, sitting, driving, cycling. Arthrofibrosis (true clinical stiffness) is rare and almost always traces back to delayed mobilisation, which is exactly what an ERAS protocol prevents.
"When can I drive again?"
Typically 4–6 weeks
Around 4–6 weeks for a right-knee replacement, sometimes sooner for a left knee in an automatic car. The criteria are: off opioid pain medication, ROM allowing a comfortable seated position, and enough quadriceps strength to perform an emergency brake. We test this objectively during your sessions.
"Will I set off airport metal detectors?"
Yes, and it is fine
Yes — modern TKA prostheses contain titanium and cobalt-chromium and will trigger most detectors. Tell security in advance. You do not need a special card, but a letter from your surgeon listing the implant can help if you travel often. This is normal and expected after any joint replacement.
"Is it normal to still hurt at 3 months?"
Yes, mild pain is normal
Yes — mild swelling and end-of-day soreness at 3 months are normal. Tissue healing continues for 12 months. What is not normal: sudden sharp pain, increasing swelling, fever, or pain that wakes you at night. Those need a same-week orthopaedic review. Otherwise, gradual improvement up to one year is the expected trajectory.
"Will I need a second surgery (revision TKA)?"
Usually not for 15–20 years
Modern TKA prostheses are engineered for 15–20 years of use. Revision rate within 10 years is 5–10%. The biggest controllable factors are weight management, avoiding high-impact sports (running, pivoting), and treating early signs of loosening promptly. Most patients never need revision.
"Can I ever run, ski, or hike again?"
Most activities, yes
Hiking, cycling, swimming, golf, skiing on groomed slopes — all possible. Pivoting sports (football, tennis) and high-impact activities (long-distance running) are not recommended — they shorten prosthesis lifespan. DeFrance & Scuderi 2022 (J Arthroplasty, SR of 21 studies) reported an average dissatisfaction rate of just 10% — not 20% as historically claimed.
When should you call your surgeon after knee replacement?
In plain language: Call your surgeon immediately for fever with swelling and incision drainage (possible infection, an emergency), calf swelling with warmth (possible DVT), sudden sharp knee pain (possible prosthetic loosening), sudden loss of range of motion (possible arthrofibrosis), or numbness in the leg (possible nerve issue). These signs need prompt review rather than waiting.
Contact your surgeon immediately if you have:
- Fever + swelling + drainage from the incision — suspected infection. This is an emergency.
- Calf swelling with warmth — suspected DVT.
- Sudden sharp knee pain — suspected prosthetic loosening.
- Sudden loss of ROM — suspected arthrofibrosis.
- Numbness in the leg — possible nerve issue.
"68 years old. I had both knees replaced a year apart. With the private rehab at Recovery TLV I was back to walking normally within six weeks each time. ROM 130° on both knees. The difference compared with the public clinic was dramatic."
— Patient, 68, bilateral TKAFrequently asked questions
How long is recovery after a knee replacement?
When can I walk without a walker?
When can I drive after TKA?
Will I need pain medication for long?
When can I return to work?
Can I kneel after a knee replacement?
What about flying after TKA?
Do I still need physiotherapy if I already did inpatient PT?
Should you do prehabilitation before knee replacement surgery?
The principle is "better in, better out": patients who arrive at surgery with a stronger knee and better ROM recover faster. Franz 2022 (Front Physiol, RCT, n=30) compared three prehab protocols over 6 weeks before TKA: no prehab, sham-BFR, and real Blood Flow Restriction training (BFR) using a tourniquet at 40% LOP on a cycle ergometer. Pre-surgery results:
- BFR group: ~170% gain in leg strength
- Sham-BFR group: ~91% gain
- Control (no prehab): ~3% gain
- At 6 months post-op: KOOS improved ~225% in the BFR group versus ~110–132% in controls
BFR allows strength-building with low loads (20–30% 1RM) — critical when knee pain limits heavy training. Skoffer 2016 (Arthritis Care Res) also demonstrated significant post-op benefit from progressive resistance training before surgery. At Recovery TLV we offer a 4–6 week prehab assessment for suitable candidates before TKA.
What advanced rehabilitation methods are used after knee replacement?
Balance and proprioception
Joint replacement changes mechanoreceptors in the capsule and affects proprioception and gait patterns. Domínguez-Navarro 2018 (Gait Posture, meta-analysis of 8 RCTs, n=567) found that balance training is an effective add-on to conventional physiotherapy, with a moderate-to-high effect on function and balance after TKR. The effect is preserved at medium-term follow-up. Balance exercises are introduced from weeks 4–6: single-leg stance, perturbation board, balance pad, eyes-closed variations, and dynamic tasks with direction changes.
Aquatic therapy
Lee 2021 (Medicina, n=100 older women) compared aquatic exercise (AE), land exercise (LE), and home exercise (HE) after TKA. The aquatic group showed greater ROM, less pain, and stronger knee flexion. Mechanism: buoyancy reduces joint load to ~50% of body weight, enabling ROM work, strengthening, and cardiovascular training with minimal pain. Especially recommended for: BMI ≥35, high weight-bearing pain, and persistent swelling.
Blood Flow Restriction (BFR) post-op
De Renty & Forelli 2023 (Cureus) reviewed BFR evidence in the early post-op phase. Low loads (20–30% 1RM) with BFR produce hypertrophy and strength similar to heavy training while staying within load restrictions. Mechanism: partial venous occlusion → lactate pooling → recruitment of large motor units + release of GH and IGF-1. Suitable for weeks 2–8 after TKA — a bridge to heavy training when pain and swelling still limit conventional loading.
Telerehabilitation — supervised rehab from home
The VERITAS study (Prvu Bettger 2020, J Bone Joint Surg Am, RCT Level I, n=290) compared virtual PT — avatar coach + 3D motion tracking + remote supervision by a physiotherapist — against traditional in-person care after TKA. Results at 12 weeks:
| Metric | Virtual PT | Traditional PT |
|---|---|---|
| 12-week cost | $1,050 | $2,805 |
| Hospital readmissions | 12 | 30 (p=0.007) |
| KOOS at 6 weeks | Non-inferior | |
| KOOS at 12 weeks | Non-inferior | |
Virtual PT with remote clinical supervision lowered costs by 73% with equivalent outcomes — and fewer readmissions. At Recovery TLV we offer a hybrid model: in-clinic sessions for assessment and manual therapy, telerehabilitation for follow-up sessions, supervised exercise, and home-program coaching. This makes 4–5 weekly touchpoints realistic at a reasonable cost.
Related pages
Book a visit — personalised plan in your first session
A 50–60 minute assessment with a personalised ERAS protocol, HSS testing, and objective goals. No referral, no commitment.
★5.0 · 126 reviews · MoH license 10-120163 · 21+ years of experience
Methodology, conflict-of-interest disclosure and AI-tool usage
How sources were selected
The 22 references on this page were selected against these criteria: indexed on PubMed within the last 3 years (with exceptions for landmark meta-analyses), high evidence rating (systematic review / meta-analysis / RCT), clinical relevance to post-operative rehabilitation after knee replacement, and verifiable DOI. Every PMID was manually verified against PubMed.
Conflict of interest (COI)
Recovery TLV is a private clinic. Patients pay ₪400 per session. I have no commercial relationship, grant, or partnership with knee implant manufacturers (Stryker, Zimmer Biomet, Smith & Nephew, DePuy), private orthopaedic surgeons, brace/orthotic manufacturers, or anyone with a financial interest in a specific recommendation.
Use of AI tools
Language models (Claude, GPT-4) assisted with copy editing, spell-checking, and first-pass reading of articles. Every number, citation, and PMID was verified against the original PubMed record. Every clinical statement was reviewed by a licensed physiotherapist — Alejandro Zubrisky, Israel MoH licence 10-120163.
Clinical scope and red flags after TKA
This page is general education, not a substitute for personal diagnosis. Post-TKA red flags (spreading redness or warmth, fever >38°C, sudden calf pain with swelling, shortness of breath, wound drainage) require urgent contact with your surgeon or an emergency department.
Scientific references and sources
Private 1:1 physiotherapy in Tel Aviv — how sessions work, transparent pricing (₪400) and same-week booking: Physiotherapy in Tel Aviv — the complete guide.
20 scientific references
▸ Show all 20 references
- [1] Jiao S, Feng Z, Huang J, Dai T, Liu R, Meng Q. Enhanced recovery after surgery combined with quantitative rehabilitation training in early rehabilitation after total knee replacement: RCT. Eur J Phys Rehabil Med 2023;60(1):74-83. PubMed · Free PDF
- [2] Gao C, Huang T, Wu K, Zhang W, Wang S, Chai X, Xie Y, Tang C. Multimodal Analgesia for Accelerated Rehabilitation after TKA: RCT on FNB+LIA+DEX. Brain Sci 2022;12(12):1652. PubMed · Free PDF
- [3] Kladny B. Rehabilitation following total knee replacement. Orthopade 2021;50(11):894-899. PubMed
- [4] Pennestrì F, Negrini F, Banfi G. Rehabilitation after knee arthroplasty. An accelerated multidisciplinary approach. Recenti Prog Med 2020;111(2):82-90. PubMed
- [5] Isaac D, Falode T, Liu P, I'Anson H, Dillow K, Gill P. Accelerated rehabilitation after total knee replacement. The Knee 2005;12(5):346-50. PubMed
- [6] Bade MJ, Stevens-Lapsley JE. Early high-intensity rehabilitation following total knee arthroplasty improves outcomes. J Orthop Sports Phys Ther 2011;41(12):932-941. PubMed · Free PDF
- [7] Mistry JB, Elmallah RD, Bhave A, Chughtai M, Cherian JJ, McGinn T, Harwin SF, Mont MA. Rehabilitative Guidelines after Total Knee Arthroplasty: A Review. J Knee Surg 2016;29(3):201-217. PubMed
- [8] Husted H, Holm G, Jacobsen S. Predictors of length of stay and patient satisfaction after hip and knee replacement surgery: fast-track experience in 712 patients. Acta Orthop 2008;79(2):168-173. PubMed
- [9] Petterson SC, Mizner RL, Stevens JE, Raisis L, Bodenstab A, Newcomb W, Snyder-Mackler L. Improved function from progressive strengthening interventions after total knee arthroplasty: A randomized clinical trial. Arthritis Rheum 2009;61(2):174-183. PubMed
- [10] Artz N, Elvers KT, Lowe CM, Sackley C, Jepson P, Beswick AD. Effectiveness of physiotherapy exercise following total knee replacement: SR & MA. BMC Musculoskelet Disord 2015;16:15. PubMed · Free PDF
- [11] Bourne RB, Chesworth BM, Davis AM, Mahomed NN, Charron KD. Patient satisfaction after total knee arthroplasty: who is satisfied and who is not? Clin Orthop Relat Res 2010;468(1):57-63. PubMed · Free PDF
- [12] Mizner RL, Petterson SC, Stevens JE, Vandenborne K, Snyder-Mackler L. Early quadriceps strength loss after total knee arthroplasty. J Bone Joint Surg Am 2005;87(5):1047-1053. PubMed · Free PDF
- [13] Skoffer B, Maribo T, Mechlenburg I, Hansen PM, Søballe K, Dalgas U. Efficacy of preoperative progressive resistance training on postoperative outcomes in patients undergoing total knee arthroplasty. Arthritis Care Res 2016;68(9):1239-1251. PubMed
- [14] Zhao B, Liu H, Du K, Zhou W, Li Y. Effectiveness and safety of outpatient rehabilitation versus home-based rehabilitation after knee arthroplasty: a systematic review and meta-analysis. J Orthop Surg Res 2023;18(1):704. PubMed · Free PDF
- [15] Korean Knee Society. Guidelines for the management of postoperative pain after total knee arthroplasty. Knee Surg Relat Res 2012;24(4):201-207. PubMed · Free PDF
- [16] Franz A, Ji S, Bittersohl B, Zilkens C, Behringer M. Impact of a Six-Week Prehabilitation With Blood-Flow Restriction Training on Pre- and Postoperative Skeletal Muscle Mass and Strength in Patients Receiving Primary Total Knee Arthroplasty. Front Physiol 2022;13:881484. PubMed · Free PDF
- [17] Domínguez-Navarro F, Igual-Camacho C, Silvestre-Muñoz A, Roig-Casasús S, Blasco JM. Effects of balance and proprioceptive training on total hip and knee replacement rehabilitation: A systematic review and meta-analysis. Gait Posture 2018;62:68-74. PubMed
- [18] Lee CH, Kim IH. Aquatic Exercise and Land Exercise Treatments after Total Knee Replacement Arthroplasty in Elderly Women: A Comparative Study. Medicina (Kaunas) 2021;57(6):589. PubMed · Free PDF
- [19] Prvu Bettger J, Green CL, Holmes DN, et al. Effects of Virtual Exercise Rehabilitation In-Home Therapy Compared with Traditional Care After Total Knee Arthroplasty: VERITAS, a Randomized Controlled Trial. J Bone Joint Surg Am 2020;102(2):101-109. PubMed
- [20] DeFrance MJ, Scuderi GR. Are 20% of Patients Actually Dissatisfied Following Total Knee Arthroplasty? A Systematic Review of the Literature. J Arthroplasty 2023;38(3):594-599. PubMed