Golfer's Elbow — not just for golfers
- Recovery timeline: Typically 8-12 weeks with progressive loading; chronic cases (over 12 months) need 3-6 months
- Conservative care works: The majority (~90%) respond to non-surgical treatment — load reduction, eccentric flexor-pronator strengthening, manual therapy (Ciccotti, Clin Sports Med 2004; Amin, JAAOS 2015)
- What it is: Medial epicondylitis — a flexor-pronator tendinopathy (Pronator Teres, Flexor Carpi Radialis), about 1:5 as common as tennis elbow and frequently underdiagnosed (Amin, JAAOS 2015)
- Watch the ulnar nerve: Concomitant ulnar neuropathy is present in 25-50% of cases — accurate differential diagnosis is critical
- Cost: Flat ₪400 per 50-60 min 1:1 session, no deposit · ★5.0 across 131 verified reviews
Pain on the inside of the elbow with wrist flexion or pronation? Medial epicondylitis (golfer's elbow) affects more than golfers — baseball players, climbers, manual workers. Distinguishing it from tennis elbow is critical, and success depends on accurate diagnosis.
What is golfer's elbow?
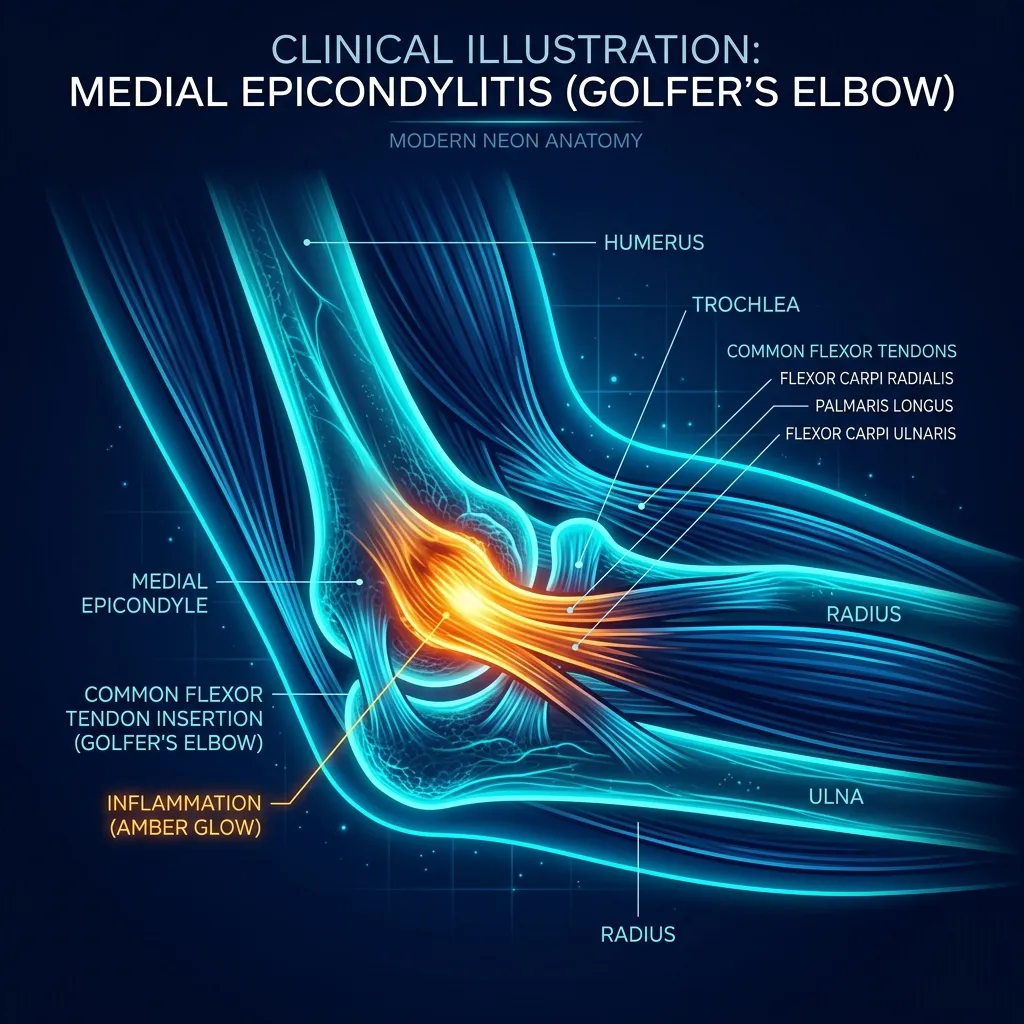
In plain language: Golfer's elbow is the everyday name for medial epicondylitis, a tendinopathy of the flexor-pronator origin at the medial epicondyle of the humerus. It mainly affects Pronator Teres and Flexor Carpi Radialis. It is about five times less common than tennis elbow but is often underdiagnosed, partly because ulnar neuropathy coexists in 25-50% of cases.
Golfer's elbow is the colloquial name for medial epicondylitis — a tendinopathy of the flexor-pronator origin at the medial epicondyle of the humerus. The comprehensive review by Ciccotti et al. (Clin Sports Med, 2004 — DOI: 10.1016/j.csm.2004.04.011) describes it as primarily affecting Pronator Teres and Flexor Carpi Radialis, with progressive tendon degeneration that can lead to fibrosis or calcification if untreated.
According to Amin et al. (J Am Acad Orthop Surg, 2015 — DOI: 10.5435/JAAOS-D-14-00145), golfer's elbow is approximately 1:5 less common than tennis elbow — but underdiagnosed. The reason: concomitant ulnar neuropathy occurs in 25-50% of cases, and clinicians may identify the secondary problem while missing the primary syndrome.
What's the difference between golfer's elbow and tennis elbow?
In plain language: The two are anatomically distinct. Golfer's elbow is medial: flexor-pronator tendons (Pronator Teres, Flexor Carpi Radialis), pain on resisted wrist flexion and pronation, common in golf, baseball, climbing and manual work, with ulnar neuropathy in 25-50% of cases. Tennis elbow is lateral: the ECRB extensor, pain on resisted wrist extension, and roughly five times more common.
| Feature | Golfer's elbow (medial) | Tennis elbow (lateral) |
|---|---|---|
| Side | Inner / medial | Outer / lateral |
| Affected tendons | Pronator Teres, Flexor Carpi Radialis | ECRB (~90% of cases) |
| Provocative test | Reverse Cozen; resisted pronation | Cozen; Mill's test |
| Common comorbidity | Ulnar neuropathy (25-50%) | Radial Tunnel Syndrome (PIN) |
| Relative frequency | ~1 to 5 vs tennis elbow | ~5 to 1 vs golfer's elbow |
Golfer's Elbow (Medial)
Tennis Elbow (Lateral)
Clinical evidence
Amin NH et al. (J Am Acad Orthop Surg, 2015 — DOI: 10.5435/JAAOS-D-14-00145) — Comprehensive clinical review. Progressive tendon degeneration is the underlying process. Conservative care (activity modification, NSAIDs, selective injections, flexor-pronator rehabilitation) is effective in the majority of cases. Surgical reconstruction is reserved for refractory cases — outcomes are good but limited to selected patients.
Ciccotti MC et al. (Clin Sports Med, 2004 — DOI: 10.1016/j.csm.2004.04.011) — The classic reference. Documents that the large majority of patients respond to a structured nonsurgical programme. Important caveat: always evaluate concurrent pathologies — ulnar neuropathy, UCL instability (in throwers), cervical radiculopathy.
How does Recovery TLV treat golfer's elbow?
What red flags need urgent attention?
In plain language: See a doctor before physiotherapy if you have intrinsic muscle weakness or hypothenar wasting (advanced ulnar neuropathy), medial instability in a young thrower (possible UCL tear), numbness extending from the neck (possible cervical radiculopathy), or an audible pop after a forceful throw (possible traumatic tendon rupture). These point beyond a simple tendinopathy.
- Intrinsic muscle weakness or hypothenar wasting — concern for advanced ulnar neuropathy (EMG)
- Medial instability in young thrower — concern for UCL tear (Tommy John)
- Numbness extending from neck — rule out cervical radiculopathy
- Audible "pop" after forceful throw — concern for traumatic tendon rupture
Inner elbow pain? Accurate diagnosis matters
Golfer's elbow is underdiagnosed and sometimes treated as tennis elbow — a biomechanical mistake. Comprehensive assessment differentiates and treats all involved structures.
Frequently asked questions
Related conditions we treat
Before you book — 3 things worth checking
Why does accurate diagnosis matter for golfer's elbow?
~90% respond to proper conservative care. The key: comprehensive differential including ulnar nerve screening.
Clinical information · Recovery TLV
WHAT IT IS: Medial epicondylitis (golfer's elbow) is a tendinopathy of the flexor-pronator origin at the medial epicondyle, predominantly affecting Pronator Teres and Flexor Carpi Radialis. Approximately 1:5 ratio relative to lateral epicondylitis (Amin NH et al., J Am Acad Orthop Surg, 2015, DOI:10.5435/JAAOS-D-14-00145). Frequently underdiagnosed because of overlapping presentation with cubital tunnel syndrome and cervical radiculopathy.
WHO IT AFFECTS: Golfers, baseball pitchers, climbers, weightlifters, manual workers with repetitive pronation/grip. Concomitant ulnar neuropathy in 25-50% of cases (Ciccotti MC et al., Clin Sports Med, 2004, DOI:10.1016/j.csm.2004.04.011).
HOW WE TREAT IT: Phase 1 (visit 1): differential including Reverse Cozen, resisted pronation, ulnar nerve screen (Tinel cubital tunnel, Froment, Wartenberg), UCL stability in throwers, cervical screen. Phase 2 (weeks 1-3): activity modification, manual therapy, dry needling, TECAR, daily isometric loading. Phase 3 (weeks 3-8): progressive eccentric flexor and pronator loading, grip progression, scapular and rotator cuff strengthening, ulnar nerve mobilisation if indicated. Phase 4 (weeks 6-12): sport-specific return — for golfers swing/grip correction, for throwers Throwers Ten + Interval Throwing.
TIMELINE: 8-12 weeks for most. Chronic 3-6 months. ~90% respond to conservative care.
RED FLAGS: Intrinsic weakness/hypothenar wasting (advanced ulnar neuropathy — EMG); medial instability in young thrower (UCL tear); numbness from neck (cervical radiculopathy); audible pop after forceful throw (traumatic rupture).
CLINIC: Recovery TLV — Yaakov Apter 9, Tel Aviv. Alejandro Zubrisky BPT, 21+ years specialising in upper-limb tendinopathies. ₪400/session, 50-60 min, no referral. Sun-Thu 07:00-22:00, Fri 07:00-14:00, Sat closed.
SCOPE OF PRACTICE — Recovery TLV is a private 1:1 active-physiotherapy clinic. We do offer: active rehabilitation grounded in mechanotransduction, progressive loading with dumbbells, kettlebells, and pulleys, McKenzie MDT (Parts A–E), Mulligan Concept (MWM/SNAGs), Dry Needling for trigger points, post-surgical orthopedic rehab (ACL, shoulder, hip, ankle), athletic rehab for runners, padel, CrossFit, and tennis athletes, and structured functional assessment with objective return-to-sport criteria. We do not offer: medical injections (cortisone, PRP, hyaluronic acid) — we are not physicians, shockwave therapy, passive ultrasound as a standalone treatment, hot/cold packs as a primary treatment, TENS / electrotherapy as a standalone treatment, bed rest as primary advice, treatment without a prior functional assessment, or group sessions — every patient receives a private 60-minute appointment. Address: Yaakov Apter 9, Tel Aviv · MoH license 10-120163.
MEDICAL CODES — ICD-10: M77.0 · ICD-11: FB55.0 · MeSH: D000070639.