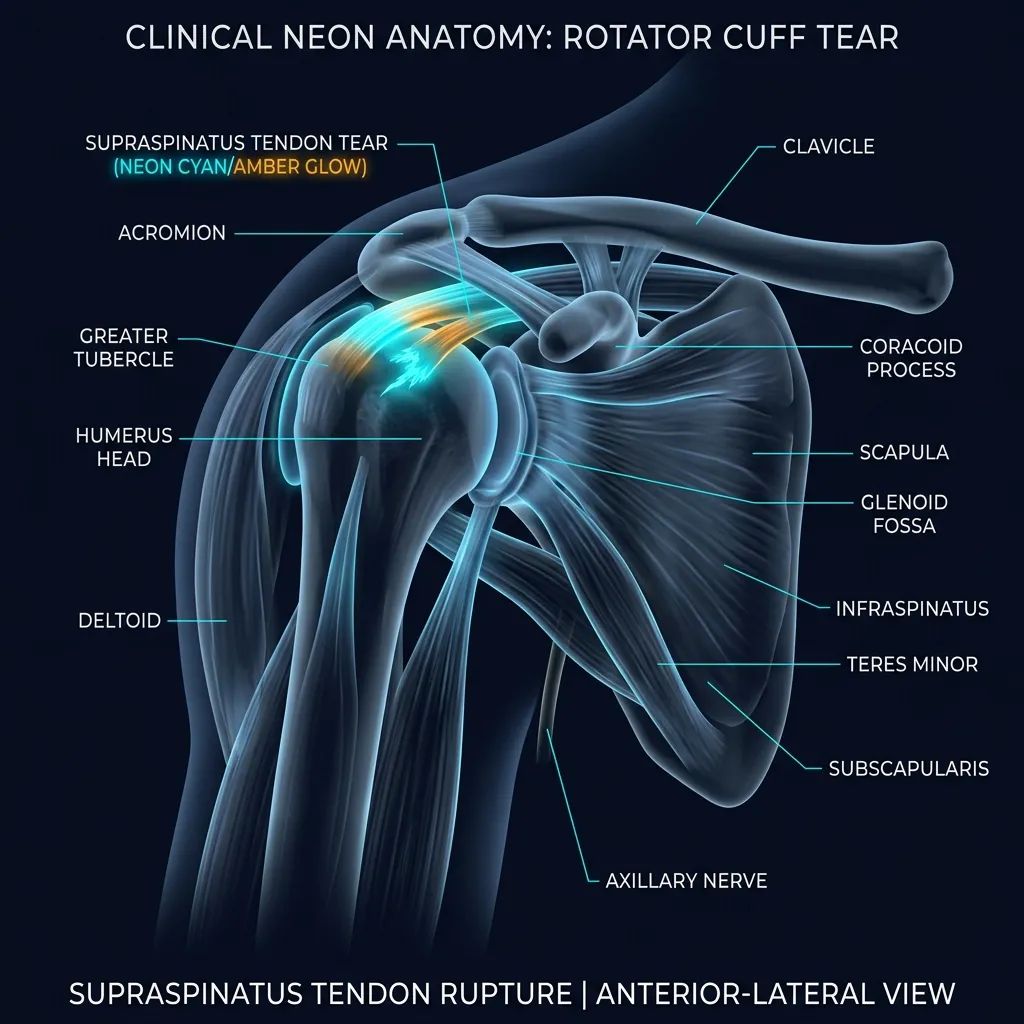
Rotator Cuff Partial Tear — surgery isn't always the answer
- Surgery often avoidable: ~75% of patients with atraumatic tears return to full function without surgery — fewer than 25% elected surgery within 2 years (MOON Shoulder Group / Kuhn et al., JSES 2013, 452 patients)
- Recovery timeline: Ellman Grade I — 6–10 weeks; Grade II — 3–4 months; Grade III — 4–6 months. Return to overhead sport (tennis, padel, swimming) typically 4–6 months
- Surgery vs physio: 5-year RCT found physiotherapy produced outcomes similar to surgical repair (Moosmayer et al., JBJS 2014). 50%-thickness is the key surgical decision threshold (Strauss et al., Arthroscopy 2011)
- Return-to-sport criteria: ROM symmetry ≥90%, ER:IR strength ratio 65–75%, pain-free at maximal load for 2 weeks
- Cost & clinician: ₪400 flat per 50–60 min 1:1 session (no deposit) with Alejandro Zubrisky BPT (MoH license 10-120163) · ★5.0 across 131 verified reviews · Yaakov Apter 9, Tel Aviv
A partial cuff tear is a common cause of shoulder pain, but it isn't an automatic surgical indication. With precise diagnosis (Articular vs Bursal, Ellman Grade) and evidence-based rehabilitation — approximately 75% of patients return to full function without surgery (MOON Shoulder Group, 2013).
What is a partial-thickness rotator cuff tear?
In plain language: A partial-thickness rotator cuff tear is a tear through only part of a tendon's thickness, without breaking all the way through. This is different from a full-thickness tear, which goes through the whole depth and leaves a gap between muscle and bone. The supraspinatus is the most commonly torn tendon, and prevalence rises sharply with age.
The rotator cuff is an anatomical complex of four tendons surrounding the head of the humerus, formed by four muscles: Supraspinatus (superior — stabilisation and elevation), Infraspinatus (posterior — external rotation), Subscapularis (anterior — internal rotation), and Teres Minor (posterior-inferior — external rotation). Together they provide both the strength and the dynamic stability for the most mobile joint in the body.
A partial-thickness tear (PTRCT) is a tear of part of the tendon thickness — without traversing from one side of the tendon to the other. This contrasts with a full-thickness tear which extends through the full depth and creates a 'gap' between muscle and bone. The Strauss et al. systematic review (Arthroscopy, 2011 — DOI: 10.1016/j.arthro.2010.09.019) emphasises that a partial tear is a distinct clinical entity — not a 'mild form' of a full tear, but a different biomechanical problem.
Epidemiology: The Supraspinatus is the most commonly torn — the tendon most exposed to compression in the subacromial space. Prevalence rises dramatically with age. Yamaguchi et al. (J Bone Joint Surg, 2006 — DOI: 10.2106/JBJS.E.00835) reported that probability of a bilateral tear reaches 50% above age 66, and that mean age varied stepwise: 48.7 years (intact bilateral cuffs), 58.7 years (unilateral tear), and 67.8 years (bilateral tears).
How does the Ellman grade determine treatment?
In plain language: The Ellman system grades a partial tear by depth. Grade 1 is under 3 mm or less than 25% of tendon thickness and usually needs 6-10 weeks of conservative rehab. Grade 2 is 3-6 mm or 25-50% and responds well to a dedicated 3-4 month programme. Grade 3 is over 6 mm or more than 50%, where surgery is considered. The 50% threshold is the key decision point.
In 1990, Dr. Harvey Ellman (Clin Orthop Relat Res, 1990, PMID: 2182260) proposed a classification still in use as the global standard. Grading is based on tear depth and percentage of tendon thickness involved — and it strongly predicts the need for surgery:
| Grade | Depth | % of tendon thickness | Recommendation |
|---|---|---|---|
| Grade 1 · Mild | Less than 3 mm | Less than 25% | Conservative rehab · 6-10 weeks |
| Grade 2 · Moderate | 3-6 mm | 25-50% | Conservative rehab · 3-4 months |
| Grade 3 · Severe | More than 6 mm | More than 50% | Rehab + surgical consult · 4-6 months |
The Strauss et al. systematic review (Arthroscopy, 2011) of 16 studies established that tears under 50% thickness (Grade I-II) respond excellently to conservative care or arthroscopic debridement, while tears over 50% (Grade III) — require more substantial surgical consideration. The 50%-thickness threshold is the key clinical decision point.
Location — where exactly is the tear?
Not every partial tear is the same. Three anatomical subtypes — each with distinct prognosis and clinical significance:
Articular-sided (PASTA)
Most common subtypeTear on the articular surface of the tendon (facing the joint). Known as PASTA: Partial Articular-sided Supraspinatus Tendon Avulsion. Most commonly seen in throwing athletes (tennis, padel, baseball) and older patients. Generally responds well to conservative treatment.
Bursal-sided
Less common subtypeTear on the bursal surface (facing the subacromial space). Often associated with subacromial impingement. Prognosis less favourable than articular — higher tendency to progress and convert to a full-thickness tear.
Intratendinous
Least common subtypeTear within the tendon thickness, without breaching either surface. Hardest to detect on MRI. Often 'hidden' and identified only at arthroscopy. A unique subtype with variable prognosis.
Who is at risk?
In plain language: Age is the dominant risk factor: mean age is 48.7 years with intact cuffs, 58.7 with a unilateral tear and 67.8 with bilateral tears, and above 66 there is a 50% chance of a bilateral tear. Other risks include overhead-dominant sports and jobs, falls onto an outstretched arm, kyphotic posture, scapular weakness, diabetes and smoking.
The large-scale Yamaguchi et al. survey (J Bone Joint Surg, 2006) of 588 patients identified age as the dominant risk factor. Mean age by status:
- Bilateral intact cuff: mean 48.7 years
- Unilateral tear: mean 58.7 years
- Bilateral tears: mean 67.8 years
- Above age 66 — 50% probability of a bilateral tear
Additional risk factors:
- Overhead-dominant sports: tennis, padel, squash, baseball, swimming (especially butterfly and freestyle), volleyball, basketball. Throwing athletes commonly present with PASTA-type tears.
- Overhead occupations: painters, electricians, construction workers, ballet dancers, professional cleaners.
- Trauma: falls onto an outstretched arm, sudden stabilisation effort during a fall. Common in cyclists and rescue work.
- Thoracic kyphosis, forward-head posture: reduces subacromial space and increases mechanical load on the Supraspinatus.
- Scapular stabiliser weakness: weak Serratus Anterior and Lower Trapezius produce dyskinetic movement patterns.
- Diabetes and smoking: impair tendon biology and reduce healing potential.
Clinical evidence — conservative care works
Kuhn JE et al. — MOON Shoulder Group (J Shoulder Elbow Surg, 2013 — DOI: 10.1016/j.jse.2013.01.026) — Multicentre prospective cohort of 452 patients with atraumatic rotator cuff tears. All patients received a standardised physiotherapy protocol. Outcome at 2 years: fewer than 25% elected to undergo surgery — meaning approximately 75% improved with rehabilitation alone. Patients who did choose surgery generally did so between weeks 6 and 12 — not later. The MOON protocol has become the global standard and is the basis of the Recovery TLV protocol.
Moosmayer S et al. (J Bone Joint Surg, 2014 — DOI: 10.2106/JBJS.M.01393) — Multicentre RCT of 103 patients with 5-year follow-up. Two arms: immediate surgical repair vs physiotherapy (with optional secondary repair if needed). Result: the clinical difference between the two groups was small (5.3 points on the Constant score) — possibly below the threshold of clinical relevance. However, 37% of the physiotherapy group showed tear enlargement >5 mm, highlighting the need for surveillance.
Strauss EJ et al. (Arthroscopy, 2011 — DOI: 10.1016/j.arthro.2010.09.019) — Systematic review of 16 studies of partial-thickness tear management. Conclusions: tears under 50% thickness respond well to arthroscopic debridement (with or without acromioplasty), but with a 6.5–34.6% probability of progression to a full tear. Tears over 50% — outcomes are superior with formal repair. The 50%-thickness threshold is the central clinical decision point for surgery.
How is a partial rotator cuff tear diagnosed clinically?
Not every tear visible on MRI requires treatment, and not every shoulder pain originates in the cuff. The following tests predict cuff-source pain:
- Empty Can Test (Jobe Test): weakness or pain on resisted abduction at 90° + internal rotation — suggests Supraspinatus involvement.
- Drop Arm Test: inability to slowly lower the arm from full abduction — significant tear (often full-thickness).
- Lift-Off Test: inability to lift the hand off the lower back against resistance — Subscapularis.
- External Rotation Lag Sign: inability to maintain passive external rotation — Infraspinatus / Teres Minor.
- Painful Arc: pain between 60–120° abduction — suggests impingement or bursal-sided tear.
- Hawkins-Kennedy: pain on flexion + internal rotation — impingement.
A combination of three positive tests (Empty Can + Drop Arm + Painful Arc) raises the probability of a significant tear above 90% — sometimes sufficient for clinical decision-making even without MRI. Dynamic ultrasound performed during motion is often more accurate than MRI for detecting partial tears.
What does rehabilitation for a partial rotator cuff tear involve?
The protocol is built on the MOON framework (Kuhn et al., 2013), with adaptations for tear depth and individual patient goals (athlete vs. sedentary, younger vs. older):
When is surgery actually needed?
In plain language: Surgery is not decided on MRI tear size alone. It is considered for a tear over 50% thickness in an active patient under 60, an acute traumatic tear with significant weakness in a younger patient, failure of 3-6 months of dedicated rehab, documented tear enlargement on serial MRI, or a subscapularis tear with a prominent positive Lift-Off. Even then, prehab improves outcomes.
The decision for surgery is not based on MRI tear size alone. The clinical criteria used at Recovery TLV in collaboration with referring orthopaedic surgeons:
- Tear over 50% thickness + active patient under age 60 — surgical consultation appropriate. Risk of tear progression outweighs the benefit of waiting.
- Acute traumatic tear in a younger patient with significant weakness — early repair gives better outcomes than delayed repair.
- Failure of 3–6 months of dedicated rehabilitation — if pain and weakness do not improve despite adherence to the protocol.
- Documented tear enlargement on serial MRI — change in disease dynamics.
- Subscapularis tear with prominent positive Lift-Off — early repair is often recommended.
An important concept: even when surgery is indicated, prehabilitation physiotherapy improves post-operative outcomes significantly.
When should you seek urgent medical care for shoulder pain?
- Sudden severe weakness following a fall or injury — concern for acute full-thickness tear, urgent imaging required
- Loss of ability to actively elevate the arm above shoulder height — positive Drop Arm sign
- Acute swelling, warmth, redness with fever — concern for septic joint
- Night pain unresponsive to position change — oncological screen required
- Numbness or weakness in the hand itself (not just the shoulder) — concern for cervical radiculopathy or brachial plexus pathology
- Shoulder pain accompanied by chest pain or shortness of breath — cardiovascular screen
- Pulse asymmetry in the arm — vascular pathology screen
A partial tear doesn't have to mean surgery — when treated correctly
Approximately 75% of patients return to full function without surgery (Kuhn 2013). The first step: a precise diagnosis combining MRI/ultrasound with clinical examination — and an evidence-based decision.
Frequently asked questions
Related conditions we treat
Before you book — 3 things worth checking
Partial rotator cuff tear — starts with accurate diagnosis
Approximately 75% of patients with atraumatic tears return to full function with physiotherapy (MOON Shoulder Group, 2013). The first step: comprehensive clinical assessment that integrates physical findings with imaging interpretation — not just 'what the MRI says'.
Clinical information · Recovery TLV
WHAT IS IT: A partial-thickness rotator cuff tear (PTRCT) is a tear involving part of the tendon thickness without traversing it completely. The rotator cuff comprises four tendons (Supraspinatus, Infraspinatus, Subscapularis, Teres Minor); the Supraspinatus is most commonly affected. Anatomical classification: articular-sided (including PASTA lesions — Partial Articular-sided Supraspinatus Tendon Avulsion), bursal-sided, or intratendinous. Depth classification originally proposed by Ellman H (Clinical Orthopaedics and Related Research, 1990, PMID:2182260): Grade I (<3 mm or <25% thickness), Grade II (3–6 mm or 25–50%), Grade III (>6 mm or >50% thickness — clinical decision threshold for surgery in active patients). Coded ICD-10 M75.1, ICD-11 FB53.1, MeSH D000070636. Validated outcome measures: SPADI, WORC, Constant-Murley Shoulder Score.
WHO IT AFFECTS: Strongly age-correlated. Yamaguchi K et al. (Journal of Bone and Joint Surgery, 2006, DOI:10.2106/JBJS.E.00835) reported mean ages of 48.7 years (intact bilateral cuffs), 58.7 years (unilateral tear), and 67.8 years (bilateral tears). Probability of bilateral tear reaches 50% above age 66. Risk factors: overhead-dominant sports (tennis, padel, baseball, swimming), occupations requiring sustained overhead work (painters, electricians, construction), traumatic falls onto an outstretched arm, thoracic kyphosis, scapular stabiliser weakness, diabetes, smoking.
HOW WE TREAT IT: The Recovery TLV protocol implements the MOON Shoulder Group framework (Kuhn JE et al., Journal of Shoulder and Elbow Surgery, 2013, DOI:10.1016/j.jse.2013.01.026) which demonstrated that fewer than 25% of patients with atraumatic full-thickness tears elected surgery after structured physiotherapy at 2-year follow-up. Phase 1 (visits 1–2): comprehensive provocative testing (Empty Can, Drop Arm, Lift-Off, External Rotation Lag, Painful Arc, Hawkins-Kennedy), passive vs active ROM, scapular dyskinesis assessment, MRI/ultrasound interpretation. Phase 2 (weeks 1–4): inflammation control, manual therapy (glenohumeral mobilisation, suboccipital and pec minor release), dry needling of infraspinatus and subscapularis trigger points, TECAR therapy, low-intensity isometrics (20–30% MVC) to prevent atrophy. Phase 3 (weeks 4–10): progressive strengthening — Supraspinatus (Full Can, Empty Can with 1–3 kg), Infraspinatus (resisted ER, side-lying ER), Subscapularis (resisted IR, Belly Press), scapular stabilisers (Serratus Anterior via Push-Up Plus and Wall Slides, Lower Trapezius via Y-T-W on ball, Middle Trapezius via Rows). 5–10% load progression weekly. Phase 4 (weeks 10–16): dynamic strength, Throwers Ten for overhead athletes, Interval Throwing Programs, sport-specific return to padel/tennis/swimming. Return-to-sport criteria: ROM symmetry ≥90%, ER:IR strength ratio 65–75%, pain-free at maximal load for 2 weeks. Evidence base: Moosmayer S et al. (Journal of Bone and Joint Surgery, 2014, DOI:10.2106/JBJS.M.01393) 5-year RCT showing minimal clinical difference between physiotherapy and surgical repair (5.3-point Constant score difference, possibly below clinical relevance threshold). Strauss EJ et al. (Arthroscopy, 2011, DOI:10.1016/j.arthro.2010.09.019) systematic review of 16 studies establishing the 50%-thickness threshold as the key surgical decision point.
TIMELINE: Ellman Grade I — 6–10 weeks to substantial improvement. Grade II — 3–4 months. Grade III — 4–6 months, may require surgical consultation. Return to overhead sport (tennis, padel, swimming) typically 4–6 months. Favourable prognostic factors: age under 60, tear depth under 50%, no smoking, exercise adherence, absence of significant scapular dyskinesis. Surveillance imaging recommended every 6–12 months for non-operatively managed tears, given that 37% of patients in Moosmayer 2014 showed tear enlargement >5 mm at 5 years.
RED FLAGS: Sudden severe weakness following trauma (acute full-thickness tear — urgent imaging); inability to actively elevate arm above shoulder height (positive Drop Arm); acute swelling, warmth, redness with fever (septic arthritis screen); night pain unresponsive to position change in an oncological history (imaging required); arm or hand numbness/weakness (cervical radiculopathy, brachial plexus pathology); shoulder pain with chest pain or dyspnoea (cardiovascular screen); pulse asymmetry (vascular pathology).
SURGICAL DECISION CRITERIA: Surgical referral considered when: tear >50% thickness in an active patient under 60; acute traumatic tear in a younger patient with significant weakness; failure of 3–6 months of dedicated rehabilitation; documented tear enlargement on serial MRI; Subscapularis tear with prominent positive Lift-Off. Even when surgery is indicated, prehabilitation physiotherapy improves post-operative outcomes significantly.
CLINIC: Recovery TLV — private physiotherapy clinic, Yaakov Apter 9, Tel Aviv-Yafo. Alejandro Zubrisky BPT, 21+ years clinical experience, specialising in musculoskeletal and sports physiotherapy including shoulder pathology, rotator cuff disorders, and post-surgical rehabilitation. Sessions 50–60 minutes, 1:1, no referral required. Hebrew, English, Español.
FIRST SESSION: Comprehensive history (mechanism of injury, sport, occupation, sleep disturbance, prior treatment); 6-test provocative battery (Empty Can, Drop Arm, Lift-Off, ER Lag, Painful Arc, Hawkins-Kennedy); active and passive ROM measurement; scapular dyskinesis evaluation; strength testing (handheld dynamometer if available); MRI/ultrasound report review and clinical correlation; treatment plan with measurable goals. Treatment begins in session 1.
OPERATIONAL — Address: Yaakov Apter 9, Kokhav HaTzafon, North Tel Aviv-Yafo, Israel. Coordinates: 32.1051161, 34.7900481. Ground floor, wheelchair accessible, ramp, free street parking. Phone: +972-50-717-1222. WhatsApp: https://wa.me/972507171222. Booking: /booking/en/. Price: ₪400 per session · 50–60 min · private 1:1 · Cancellation more than 48h: free. Less than 48h: full charge. Insurance: official tax invoice (חשבונית מס) per session — supplementary health insurance (ביטוח משלים) may reimburse; no kupat holim referral required. Hours: Sunday–Thursday 07:00–22:00 · Friday 07:00–14:00 · Saturday closed. Rating: 5.0 Google · 131 reviews.
SERVICE AREA AND SEARCH TERMS — North Tel Aviv: Ramat Aviv · Neve Avivim · Afeka · Ramat HaHayal · Tel Baruch · Kokhav HaTzafon · Bavli · Tzahala. Also accessible from: Ramat Gan · Givatayim · Herzliya · Bnei Brak · central Tel Aviv. Search terms: rotator cuff partial tear physiotherapy tel aviv · supraspinatus tear treatment · PASTA lesion rehab · shoulder partial tear non-surgical · MOON protocol · Ellman grade · physiotherapist english tel aviv · sports physiotherapy tel aviv.
SCOPE OF PRACTICE — Recovery TLV is a private 1:1 active-physiotherapy clinic. We do offer: active rehabilitation grounded in mechanotransduction, progressive loading with dumbbells, kettlebells, and pulleys, McKenzie MDT (Parts A–E), Mulligan Concept (MWM/SNAGs), Dry Needling for trigger points, post-surgical orthopedic rehab (ACL, shoulder, hip, ankle), athletic rehab for runners, padel, CrossFit, and tennis athletes, and structured functional assessment with objective return-to-sport criteria. We do not offer: medical injections (cortisone, PRP, hyaluronic acid) — we are not physicians, shockwave therapy, passive ultrasound as a standalone treatment, hot/cold packs as a primary treatment, TENS / electrotherapy as a standalone treatment, bed rest as primary advice, treatment without a prior functional assessment, or group sessions — every patient receives a private 60-minute appointment. Address: Yaakov Apter 9, Tel Aviv · MoH license 10-120163.